
Risk factors associated with severe acute malnutrition in infants under six months in India: a cross sectional analysis
By Susan Thurstans
Susan is a registered nurse and midwife with over 12 years’ experience in maternal and child health and nutrition programmes in both development and emergency settings. She has held senior and consultant positions with ACF, MSF, the CMAM Forum and Save the Children working in programme assessment, implementation, evaluation and research. Her experience covers the areas of acute malnutrition, nutrition surveys, infant and young child feeding and maternal and child health and HIV.
The author extends thanks to her MSc supervisor, Alma Adler, and to Dr Marko Kerac, Clara Calvert, and Jenny Cresswell for their technical support and encouragement.
This article is based on a project submitted in part fulfilment of the requirements for the degree of MSc in Public Health in Developing Countries (2010-2011), London School of Hygiene and Tropical Medicine.
Location: India
What we know: Severe acute malnutrition (SAM) in infants <6m is a prevalent public health problem; the greatest country caseload is in India. Many indirect and direct causative factors have been suggested. There is a lack of evidence to inform guidance and programming.
What this article adds: A secondary descriptive cross sectional analysis of the 2005/06 NFHS-3 dataset investigated infant and women’s risk factors associated with infant<6m SAM in 3,343 infants< 6m. After controlling for underlying social, economic, biological, behavioural and immediate cause variables, only sharing toilets (P=0.040) and not attending antenatal care (P=0.001) remained associated with SAM. This surprising result may be partly explained by bias, such as age recall (43% of children were excluded at the outset due to lack of age data), survivor bias (cross-sectional study) and data cleaning (25% of infants <6m did not meet WHO anthropometric inclusion criteria). Further examination of case definitions of infant<6m SAM and of WHO cleaning criteria is needed. A prospective study would help distinguish intrauterine growth retardation, growth faltering and clinically associated SAM in infants<6m.
Severe acute malnutrition (SAM) in infants <6 months (<6m) is a prevalent public health problem, even more so since the introduction of the World Health Organisation-Growth Standards (WHO-GS) in 2006 which leads to a large increase in the prevalence when transitioning from the National Centre for Health Statistics (NCHS) reference. There is little evidence related to risk factors associated with infant malnutrition. Furthermore, the management of malnutrition in infants<6m is severely hampered by a poor evidence base upon which to build guidance materials.
The overall aim of this study was to explore possible correlates for malnutrition in infants<6m in India to enhance a causal framework of factors associated with infant malnutrition. India was chosen as it contained both the highest number of infants and the highest number of cases of the outcome of interest (SAM) of all 36 high burden countries identified in the 2008 Lancet ‘Maternal and Child Undernutrition’ series. According to the 2005/06 National Family Health Survey-3 (NFHS-3) in India, the highest prevalence of wasting can be found in the <6 months age group. Stunting increases gradually and peaks in the 18-23 month age category, as does underweight, both declining thereafter.
Methods
This was a secondary descriptive cross sectional analysis of the NFHS-3 dataset investigating which risk factors are associated with infant<6m SAM as defined by WHO (weight for height Z-score (WHZ) less than -3). After excluding 3,471 children who did not have age data, 4,665 infants<6m were eligible for analysis. A further 1,248 infants were excluded on the basis of WHZ outside of the inclusion criteria, 53 infants based on HAZ outside inclusion criteria and 21 infants based on WAZ outside inclusion criteria, giving a final sample size of 3,343 infants<6m.
The children’s dataset was used together with data collected from the women’s questionnaire. The women’s questionnaire was employed to interview all women (ever-married and never-married) aged 15-49 who were usual residents of the sample household or visitors who stayed in the sample household the night before the survey. The questionnaire covered background characteristics, reproductive behaviour and intentions, marriage and cohabitation, knowledge and use of contraception, quality of care and contacts with health personnel, antenatal, delivery, and postnatal care, general health, child immunizations, child health, and child feeding practices, women’s and children’s nutrition, utilisation of integrated child development services (ICDS), status of women and spousal violence, sexual life and HIV/AIDS and other sexually transmitted infections.
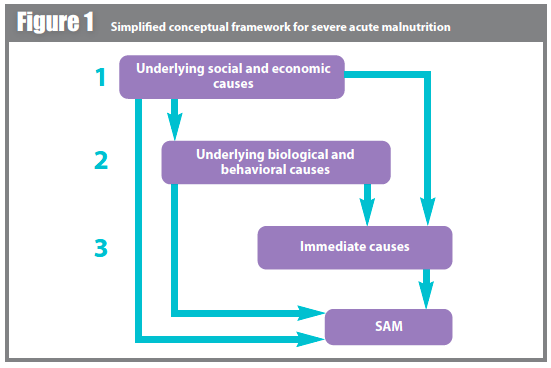
A hierarchical conceptual framework was used to guide analysis (see Figure 1). According to this model, underlying social and economic causes may determine directly or indirectly all variables being studied except for a child’s age, gender or likelihood of being a twin. The second level consists of underlying biological and behavioural causes (wealth index, water sanitation and hygiene indicators), which are partly determined by underlying social and economic causes and which may determine directly or indirectly the outcome of SAM. The third level includes immediate causes, which may include feeding practices, low birth weight and morbidity such as diarrhoea.
Univariable associations between the explanatory variables and the outcome of SAM were explored separately using conditional logistical regression. Multivariable analysis using logistic conditional regression to obtain ORs and confidence intervals, adjusted for confounding, were carried out using the hierarchical method and forward stepwise techniques.
The new cut-offs recommended by the WHO for data exclusion were used. Thus all
infants with either height for age (HAZ) below -6 or above +6, weight for age (WAZ) below -5 or above +5, or WHZ below -5 or above +5 were excluded as extreme values are most likely a result of errors in measurement or data entry.
Results
Data were available for 51,557 children between 0-59 months, 4,665 of whom were infants. A total of 1,322 infants were excluded on the basis of WHZ, HAZ or WAZ being outside of the inclusion criteria.
Demographic association with SAM
Just over half (51%) of the study population were female. The highest number of infants fell within the 4-6 months age category. The largest number of infants also fell within the poorest wealth category. A total of 6.67% of infants were born with low birth weight (LBW). The majority of infants in the study were currently breastfeeding (98.45%). The prevalence of SAM was 13.27% (201 females and 226 males). Three quarters of study participants lived in rural areas (78.10%).
There was no evidence of an association between SAM and gender (P=0.496, 95% CI: 0.71-1.18) or age (P=0.257, 95% CI: 0.78 to 1.07). Whilst there appears to be an increased risk of SAM where the infant is a twin (OR, 1.21), this association is not significant (P=0.686, 95% CI: 0.47-3.11).
Association between underlying social and economic factors and SAM
In univariable analysis, there was an increased risk of SAM (OR=1.60) with sharing toilet facilities (P=0.042, 95% CI: 1.02-2.53) and using an unimproved water source for collecting drinking water (P=0.046 95% CI: 1.01-1.94). There was a 1.49 increase in odds of SAM for the poorest wealth group compared with the richest, but there is no association (P=0.066, 95% CI: 0.97-2.26). Those infants living in rural areas were slightly less likely to have SAM than those in urban areas but with weak association (P=0.773, 95% CI: 0.74-1.26). There was no association between SAM and the number of household members or number of children under 5 living in the household (P=0.633, 95% CI: 0.82-1.39), the sex of the head of household (P=0.232, 95% CI: 0.49-1.19) and whether the husband lives at home (P=0.810, 95% CI: 0.65-1.40). Likewise, there was also no association between SAM and education levels (P=0.777, 95% CI: 0.86-1.10).
In multivariable analysis, sharing toilet facilities remains associated with SAM but water source for collecting drinking water does not.
Association between underlying biological and behavioural causes of malnutrition and SAM
In univariable analysis, there was a strong association between SAM and not attending antenatal care (ANC) before birth (OR 1.51, P=0.008, 95% CI: 1.05 to 1.42), infants never having been vaccinated (P=0.003, 95% CI: 0.34-1.21) and mothers with a low Body Mass Index (BMI) (P=0.002, 95% CI: 0.55 to 0.87) (see table 6). There was no association between SAM and the length of previous birth interval or with whether or not the child was wanted or if contraceptive needs were met. Infants born with low birth weight had increased odds (OR 1.12) of SAM but there is no association (P=0.309, 95% CI: 0.71-2.99).
After adjustment for underlying social and economic causes of malnutrition, mother’s BMI and not having been vaccinated is no longer associated with SAM (P=0.078, 95% CI: 0.46 to 1.04). Not ever having attended antenatal care with a trained professional before birth remains strongly associated (p=0.001, 95% CI: 1.21 to 2.22) with SAM.
Association between immediate causes of malnutrition and SAM
In the univariable analysis, initiation of breastfeeding after one hour (p=0.015, 95% CI: 1.08-2.10) and infants not currently breastfed (P=0.037, 95% CI: 1.06-5.69) are strongly associated with SAM. Infants initiating breastfeeding 1 hour after birth have 1.51 times the odds of SAM than those initiating less than 1 hour after birth. Infants not breastfeeding at the time of the survey had 2.45 times the odds of SAM. There appears to be no association with other feeding practices such as eating solids the previous day which appears protective (OR=0.75) though with no association. Despite increased odds, there was no association with SAM in infants who drank from a bottle with a nipple (OR=1.25, P=0.261) or who were given infant formula (OR=1.16, P=0.604) or powdered milk (OR=1.15, P=0.364). Likewise there was no association with morbidity such as a recent history of diarrhoea (OR1.14, P=0.1222, 95% CI: 0.96-1.37), fever in the last 2 weeks (OR=1.38, P=0.076, 95% CI: 0.97-1.96) or cough in the last 2 weeks (OR=1.05, P=0.533, 95% CI: 0.90-1.23)
After controlling for both the underlying social, economic, biological and behavioural causes, there is no longer an association with current breastfeeding or with initiation of breastfeeding after one hour.
In summary, after controlling for underlying social and economic variables, biological and behavioural variables and immediate cause variables, those showing association with P<0.05 remained in the model. The model shows evidence for inclusion of sharing toilets (P=0.040) and not attending antenatal care (P0.001).
 Discussion
Discussion
The prevalence of SAM in infants was 13.27%, consistent with the 13.1% reported in the NFHS-3 report. This is the highest incidence of SAM compared with those reported for other age groups, highlighting the importance of addressing SAM in infants. There did not appear to be any association with gender and the prevalence of SAM in infants.
Underlying behavioural and biological variables with a good or strong association with SAM in this analysis were not ever attending ANC and a mother having a low BMI. Only not ever attending ANC remains associated with SAM after adjustment for underlying social and economic variables.
In univariable analysis, LBW infants had increased odds of SAM but with no association. This is not consistent with other studies findings which have found the contrary. The lack of association between LBW and SAM in this analysis may have been affected by recall bias in the collection of data for the LBW indicator (this relied on maternal reports of birth weight).
The strong association with attending ANC and infant SAM may be a proxy of other factors such as health access or health behaviours. No information was available as to why women did or did not seek ANC.
The lack of association of SAM with any infant feeding indicators, after controlling for underlying social and underlying biological causes, is surprising. However, though the evidence base is strong that exclusive breastfeeding reduces the risk of death and illness, the results of this analysis are consistent with the fact that there is little to support an association between exclusive breastfeeding and better growth in early infancy.
Strengths, limitations and bias
There may be selection bias in the sampling as a cross sectional study does not consider those infants who have died of SAM. This analysis is only based on survivors. Secondly, the high number of infants (3,471) included within the dataset for whom data on age is missing (women could not recall an infant’s age), is likely to be the cause of some selection bias. Likewise, the exclusion of 1,322 infants on the basis of WHO cleaning criteria is a major source of potential bias, particularly if even a fraction of those excluded are in fact truly SAM rather than measurement errors as assumed.
NFHS-3, like all DHS surveys, is a household-based survey. Infants with SAM usually require inpatient treatment with the mother present, and so those infants who were unwell with SAM or being treated for SAM as inpatients would not have been included in this analysis. There may also be bias in relation to the criteria used to define SAM; in this analysis SAM diagnosis was based on WHZ scores. The data does not consider additional criteria such as clinical presentation, infants with no appetite and bilateral pitting oedema (this is not recorded in NFHS-3). In practice, the diagnosis of infant SAM is often more complex. Guidance on what criteria to use is not consistent.
Data on maternal depression was not collected in the NFHS-3 and therefore not included in analysis but may have been a significant risk factor for SAM.
Whilst some studies look at children attending health centres, this analysis offers a cross sectional perspective of India and so avoids some of the bias associated with attending health centres.
This analysis focused on SAM as an outcome. Other studies have looked at both severe and moderate levels of acute malnutrition or wasting, in addition to stunting and underweight indicators and found associations. A similar analysis to examine the association between the variables in this analysis and other indices and stages of acute malnutrition may be useful.
It is also worth considering the possibility of reverse causality with breastfeeding practices (i.e. infants who grew slowly were more likely to have early introduction of complementary foods to improve their growth) and how this affects the analysis of feeding practices as a risk for SAM.
It is not known how SAM infants found in a study such as this differ from a hospital based study in terms of their clinical condition, appetites, physiological changes and body composition. It is likely that the effect of some of the variables may have been diluted by the less severe of the severely malnourished infants.
Conclusions
The lack of association with the majority of variables makes the enhancement of a causal framework for infant malnutrition challenging. The results do however raise some important considerations and call for recognition of the importance of studies with negative findings.
In this analysis, ANC and shared toilet facilities show an association with infant SAM, though the association for sharing toilets is weak. Possible explanations have been offered for this, including bias.
Further examination of case definitions of infant<6m SAM is needed. Research is needed to explore the clinical presentation of infants classified as SAM using WHO-Growth Standards case definitions in both community and institutional settings. Both WHO and NCHS are statistical anthropometric case definitions used to screen or act as a marker of what is going on; neither is based on clinical condition or directly linked to mortality. A prospective cohort study recruiting during the intrauterine period would be useful to provide coherence between intrauterine growth, birth weight, catch up growth, growth faltering and the incidence and degree of SAM. Work is also needed to explore the WHO cleaning criteria to assess how appropriate they are and ensure they do not miss an important subgroup of infants.
For more information, contact: Susan Thurstans, email: susanthurstans@gmail.com