
Development and pilot testing of the Maternal Opportunities for Making Change (MOM-C) screening tool
 By Scott Ickes and Alex Lea
By Scott Ickes and Alex Lea
Scott Ickes is Assistant Professor at the College of William and Mary Department of Kinesiology and Health Sciences, Williamsburg, VA, USA
Alex Lea is a Medical Student at the Medical College of South Carolina at Greenville, 607 Grove Road Greenville, SC, USA
We wish to thank Sarah Martin for assistance with this article, and to the translators and mothers in the Byokulia Bisemeye mu Bantu (BBB) programme for their time and willingness to participate in this study.
Background and purpose
Scaling up essential nutrition interventions, like ready-to-use foods (RUFs) and complementary feeding education in the context of moderate acute malnutrition, holds great potential for reducing child undernutrition. Discourse about how to effectively increase coverage of such interventions is often focused on strengthening delivery systems and dissemination through community health workers. However, successful implementation of these interventions requires considerable action by caregivers, almost always mothers. Programmes often lack important information about maternal factors, which can be important for informing educational approaches.
The purpose of the Maternal Opportunities for Making Change (MOM-C) screening tool is to provide community health workers and programme designers with brief information about mothers enrolled in the programme. This tool seeks to understand underlying factors that may affect women's abilities to respond to nutrition interventions.
Tool development and pilot
The MOM-C tool was developed and based on a larger survey that was used for research purposes in 2014 (results not yet published). This abbreviated screening tool (see Box 1 has been tested at the Nyahuka Health Centre, Bundibugyo, Uganda in June and July 2015 within the context of a community-based nutrition programme called Byokulia Bisemeye mu Bantu, or BBB. The programme, which operates under World Harvest Mission, aims to provide nutritional and agricultural education, as well as RUF supplements, to families with underweight children aged 6 to 59 months. The results are being used to help the nutritional education approach of the work.
The tool covers five domains: experience with the BBB supplemental feeding programme, infant and young child feeding education, social support, psychological wellbeing and decision-making (Table 1). The first objective was to assess whether or not mothers have difficulty feeding the BBB food to the child enrolled in the programme and if so, what the reasons for these difficulties were. Participants were then asked about whether the programme education was helpful for them to make changes in how they feed their child or if making these changes remained difficult. If the respondent replied that it was difficult to make these changes, possible reasons for these difficulties were proposed in order to assess the source of difficulty, ranging from lack of money to purchase foods to whether or not the child likes the food that is prepared by the mother. To assess social support, the participant was asked questions about who supports them in their day-to-day life as they care for their children and how satisfied the mother was with the support that was provided. Psychological well-being was assessed through determining a mother’s satisfaction with their life, access to food and their feelings of safety in the community in which they lived. The final section of the survey was used in an attempt to understand what influences might affect a mother’s decision making and to what extent a mother has control over her own decision- making process regarding her child’s health and nutrition.
Pilot Testing
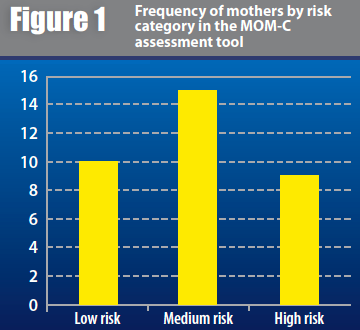
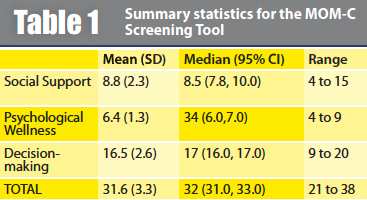
From June to July 2015, the MOM-C tool was pilot tested among 34 mothers who were currently or recently enrolled in the BBB programme. Survey results were tabulated across three domains (Social support, 6 questions, 15 possible points; Psychological Wellness, 3 questions, 12 possible points; and Decision-making 6 questions, 24 possible points) for a highest total possible score of 51, and lowest possible score of 12. Scores ranged from 21 to 38, with a mean (standard deviation) of 31.65 (3.31). We developed three risk categories: low risk (total score 12-29), medium risk (total score 30 to 32), and high risk (above 33 to 51), displayed in Figure 1. Table 2 presents the summary statistics for each sub-domain and the overall MOM-C screening tool.
Next steps for programme implementation
Following further refining of this tool, the programme will regularly adopt this screening questionnaire to assess maternal opportunities for making change at the time of programme enrolment to better understand the challenges mother face in each cohort of the programme, and to screen for mothers who are particularly vulnerable to a context of low agency, as assessed through the measured variables in this tool. Future educational messages, including programme dramas will emphasise decision-making capabilities and ways that women can advocate for and receive greater support. The programme will also encourage male partner attendance at education sessions, which will be designed to engage both partners in dialogue about issues related to women’s decision-making. Future research directions will examine the associations between levels of risk, identified in the MOM-C tool, with baseline nutritional status, biologic (e.g. growth) and behavioural (feeding practices) responses to nutrition programmes.
For more information or if you would like to pilot this tool in a different context, email: Scott Ickes