
Mothers understand and can do it (MUAC)
 Summary of research1
Summary of research1
Location: Niger
What we know: Community based management of SAM often relies on anthropometric screening by Community Health Workers. Training includes measurement of mid-point of the upper, left (non-dominant) arm.
What this article adds: In a rural setting in Niger familiar with MUAC screening, mothers given minimal training adequately performed and interpreted MUAC on their own young children. Results were comparable with Community Health Workers. Further findings suggest that the choice of arm and exact location of the tape on the upper arm are not important for screening children; it is likely the choice of arm remains relevant when measuring adolescents and adults. Frequent screening by mothers would allow early diagnosis and treatment of SAM in their children.
Community based management of severe acute malnutrition (SAM) often relies on Community Health Workers (CHW), who may be unpaid volunteers, to conduct the anthropometric measurements of children being screened and treated for SAM. Currently this requires training, standardisation testing, and follow-up; motivation and retention of these staff may also be problematic. In training to perform a mid upper arm circumference (MUAC) measurement, a CHW must learn to use the left arm and to measure and mark the mid-point of the upper arm, between shoulder tip and elbow.
The hypothesis of a recently published study is that mothers with minimal training can measure MUAC to classify the nutritional state of their children. The study hypothesis was tested in two villages in rural Niger. The rationale for teaching mothers to perform MUAC is to achieve an early diagnosis of SAM, which if acted upon in a timely manner, would decrease mortality and morbidity related to malnutrition, reduce programme costs due to shorter treatment times and lower the proportion of children requiring expensive in-patient care for SAM with complications. If mothers are able to screen their own children for malnutrition using MUAC, this may have implications for scaling up community based management of acute malnutrition (CMAM).
The study was performed between September 2011 and April 2012 in the community meeting places in two villages in Mirriah, a rural district in the Zinder region in southern Niger. There were 54 mothers with one of their children in the first village (Magema) and 49 mothers with one of their children in the second village (Berberkia). It was conducted by the Alliance of International Medical Action (ALIMA) and its local non-governmental organisation (NGO) partner BEFEN (Bien Etre de la Femme et de l’Enfant). UNICEF colour-coded and numbered MUAC tapes, calibrated in 1 mm gradations, were used for all phases of the study.
The manager of the CHW employed by BEFEN, who is well known in both villages, explained the purpose of the study to the village chiefs, elders and leaders. In each case, an independent scribe was used, recording the consent and the colour class determined by the mother, and also noting the MUAC value in millimetres.
The planned study method had involved going from home to home, and performing a five minutes training session for each mother, however this proved impossible. In both villages, once the objective of showing mothers how to perform MUAC classifications had been explained to the village chief and other leaders, it was considered to be so important that they insisted on calling an immediate meeting of the villagers. Mothers and children formed a seated group around the investigators, circled by the older girls who stood to obtain a good view, with the men and boys standing behind. Each mother did one MUAC measurement on the left arm, followed directly by one MUAC measurement on the right arm of their child. The mother called out the colour classification (e.g. “Red”) and this was noted down by the investigator. This was then repeated by an experienced CHW testing the right and then the left arm of each child, having measured the midpoint according to current recommendations. All the mothers in both villages wished to participate, however only one child from each mother was accepted into the study. Any child identified with SAM was referred to the local CMAM programme (which was run by BEFEN).
In the statistical analysis, cross-tabulations were used to investigate the agreement between mothers’ results and the CHW reference measure. The Weighted Kappa was used as a numeric summary of inter-rater agreement between two raters or methods, beyond that which would be expected by chance. Kappa is a measure of agreement, standardised along a -1 to 1 scale, where positive numbers indicate agreement, with 1 being perfect agreement; negative numbers indicate disagreement, with minus one being total disagreement; and zero indicating agreement expected by chance.
The Weighted Kappa was used because of the ordinal nature of classifications (i.e. SAM is more serious than moderate acute malnutrition (MAM), which is more serious than normal nutritional status). As a guide, the level of agreement demonstrated by Weighted Kappa values is: 0.0-0.2 ‘slight’; 0.21-0.40 ‘fair’, 0.41-0.60 ‘moderate’, 0.61-0.80 ‘substantial’ and 0.81-1.00 ‘almost perfect’. The mothers’ sensitivity; specificity; and negative and positive predictive values (NPV and PPV) using the MUAC screening for SAM were calculated using the CHW measurements as the reference result.
Results
The study showed that mothers given minimal training can perform and interpret MUAC on young children in a village setting. It suggests that the choice of arm and exact location of the tape on the upper arm are not important for screening.
Importantly, all children misclassified as not having SAM, were nevertheless classified as MAM and none were considered ‘normal’; thus classification errors occurred at the classification boundaries. Classification by mothers measuring the mid-point of the upper arm determined by eye, showed an accuracy of 86.4% – 88.4% in GAM (MUAC < 125mm) and 94.2% – 95.6% in SAM (MUAC < 115mm), compared with the current standard of the CHW classification. Roll-out of MUAC, done by mothers in the home, would involve small group learning with each mother able to practice under supervision. This would be expected further to improve the quality of the screening. There was very low inter and intra- observer variability and high levels of agreement achieved between the current standard (results from CHW), compared with mothers with minimal training. The study was conducted in free living village populations with a lower prevalence of SAM than a programme setting. This is the environment where scaled up CMAM will occur, with mothers screening their own children for malnutrition.
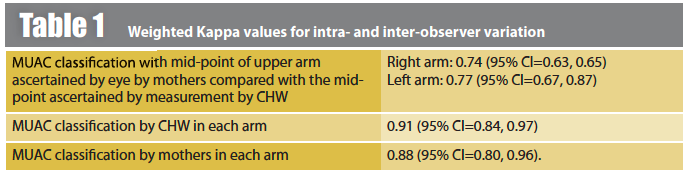
The Weighted Kapa values for MUAC classification by mothers compared to CHWs, and the variation in MUAC classification in left v right arms for both mothers and CHWs, is shown in Table 1. The observed Kappa values are consistent with excellent agreement between mothers and CHW. The Weighted Kappa values for inter-observer variation for the interpretation of classical physical signs elicited in clinical medicine are frequently less than 0.50. For example, raised respiratory rate (K=0.25), central venous pressure (K=0.3), bronchial breath sounds (K=0.32). These errors reflect variations between clinicians, patients and the circumstances at the time of the examination. Such errors can be reduced by increased standardisation of the test method and by increasing the number of times the test is performed.
It is proposed that MUAC class rather than MUAC measurement is used by mothers for active case-finding in the home. This could be facilitated by the use of broader, colour-banded MUAC straps. Numberless colour-banded MUAC tapes have been available for many years. One advantage of using a colour (red, yellow or green) for MUAC classification is that children of illiterate and /or innumerate mothers are not disadvantaged. Female literacy in the 15–24 year age group in Niger is estimated at 23%, although this is expected to be lower in rural areas.
The use of numbered MUAC tapes could only be required for monitoring response to treatment in therapeutic feeding programmes but this approach needs validation. Numbered MUAC tapes may be useful also in nutritional anthropometry surveys or surveillance systems that estimate prevalence of SAM using the PROBIT method.
 Community leaders were keen for local women to learn the skill. In contrast, men were not interested in learning the skill, while adamant that the women should learn. Mothers who had completed the task were observed to help other mothers perform the MUAC classification and the enthusiasm of girls (i.e. the next generation of mothers) to participate was striking. A future can be envisaged in which mothers in every home where childhood malnutrition is a risk are familiar with, and empowered to screen their children. Even in the most functional CMAM programme, it is unusual for children to be screened more than once a month. Repeated screening with MUAC, if a mother is concerned about her child’s health, will increase the likelihood of early diagnosis, even if the initial screen classified the child incorrectly. Training mothers to perform MUAC could provide the most timely and proximal diagnosis of malnutrition in their young children. Furthermore, programmes could be designed to facilitate mothers monitoring their children once entered into a CMAM programme, to reduce the number of repeat visits, often at great distance on foot, to the treatment centre, and increase retention in the programme, although this approach has not yet been validated. Advanced SAM is associated with complications, which often require hospital admission or cause death. Earlier diagnosis, when the MUAC has just passed the threshold for intervention, should support prompt entry into treatment programmes. This will lead to reduced mortality and length of stay, and favourable community impressions will lead to early treatment and in turn high cost-effectiveness. Giving mothers more autonomy in monitoring the nutritional status of their children may provide the tipping point in scaling up CMAM programmes.
Community leaders were keen for local women to learn the skill. In contrast, men were not interested in learning the skill, while adamant that the women should learn. Mothers who had completed the task were observed to help other mothers perform the MUAC classification and the enthusiasm of girls (i.e. the next generation of mothers) to participate was striking. A future can be envisaged in which mothers in every home where childhood malnutrition is a risk are familiar with, and empowered to screen their children. Even in the most functional CMAM programme, it is unusual for children to be screened more than once a month. Repeated screening with MUAC, if a mother is concerned about her child’s health, will increase the likelihood of early diagnosis, even if the initial screen classified the child incorrectly. Training mothers to perform MUAC could provide the most timely and proximal diagnosis of malnutrition in their young children. Furthermore, programmes could be designed to facilitate mothers monitoring their children once entered into a CMAM programme, to reduce the number of repeat visits, often at great distance on foot, to the treatment centre, and increase retention in the programme, although this approach has not yet been validated. Advanced SAM is associated with complications, which often require hospital admission or cause death. Earlier diagnosis, when the MUAC has just passed the threshold for intervention, should support prompt entry into treatment programmes. This will lead to reduced mortality and length of stay, and favourable community impressions will lead to early treatment and in turn high cost-effectiveness. Giving mothers more autonomy in monitoring the nutritional status of their children may provide the tipping point in scaling up CMAM programmes.
In Niger, international and more recently national NGOs (eg BEFEN and Forum Santé
Niger (FORSANI)) have been running nutrition programmes for more than eight years. This may explain why mothers and communities embraced the idea of doing MUAC themselves; this may not be the case in contexts unaccustomed to nutrition programmes. Widespread dissemination of MUAC tapes may be an important step in raising community awareness of malnutrition.
The study reported here collected data on children under five years of age and the results may apply only to this age-group. The choice of arm on which MUAC is measured is likely to be important in adolescents and adults in whom the MUAC of the dominant arm is generally larger than the MUAC of the non-dominant arm. Some programmes (e.g. supplementary feeding programmes) admit both children aged under five years and adults (mostly pregnant and lactating women with a MUAC below a threshold between 210 mm and 230 mm). Training and supervision of programme workers should continue to emphasise different procedures are used when measuring children and adults.
This study demonstrates that mothers can classify their children by MUAC, and it suggests MUAC done regularly by mothers should become the focal point for efforts to scale-up CMAM.
Footnotes
1Blackwell N et al (2015). Mothers understand and can do it: a comparison of mothers and community health workers determining mid-upper arm circumference in 102 children aged from 6 months to 5 years. Archives of Public Health. http://www.archpublichealth.com/content/73/1/26