
Experiences of the Sustainable Nutrition and Agriculture Promotion (SNAP) programme in the Ebola response in Sierra Leone
 By Sibida George and Georgia Beans
By Sibida George and Georgia Beans
 Sibida George is Team Leader with International Medical Corps/ SNAP and is based in Sierra Leone.
Sibida George is Team Leader with International Medical Corps/ SNAP and is based in Sierra Leone.
Georgia Beans is the Chief Of Party with ACDI-VOCA/SNAP based in Sierra Leone.
The authors would like to acknowledge USAID/Food For Peace; Jennifer Burns Senior Development Nutritionist, International Medical Corps; and Caroline Abla, Director, Nutrition and Food Security, International Medical Corps.
Location: Sierra Leone
What we know: Disease outbreaks have nutritional consequences for the individual affected and depending on the disease, for the wider community.
What this article adds: An outbreak of ebola disease in West Africa in 2014 proved a public health emergency of international concern. Existing capacity and typical programme approaches to access those affected were severely challenged. The 5 year Sustainable Nutrition and Agriculture Promotion (SNAP) programme adapted to respond to the crisis in its affected rural areas of operation. Redirected food aid to quarantined patients, self-screening by MUAC of children by lead mothers, and focus of mother child groups on essential hygiene actions were some of the adaptations. Transition to more routine programming is underway.
Background
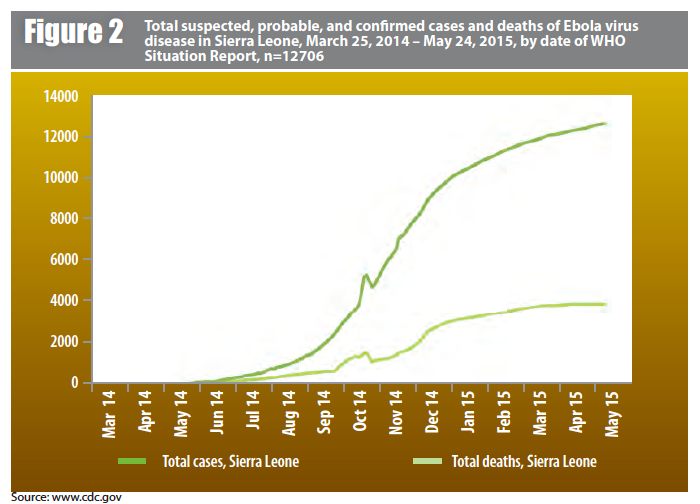
The Ebola virus disease (EVD) in West Africa broke out in Sierra Leone in May 2014. As the EVD spread, it was declared a public health emergency of international concern by the World Health Organisation (WHO) (8 August 2014). In Sierra Leone, a state of emergency (SOE) was declared on 31st July 2014 and was characterised by movement restrictions, closure of schools and learning institutions, banning periodic markets, public gatherings and avoiding body contact including handshakes. Sierra Leone has recorded 8,603 confirmed cases of EVD and 3,540 deaths including a significant number of health care professionals.
The fear of EVD disease, coupled with the restrictions under the SOE within the country and the timing during the peak agricultural season, impacted negatively on the country’s economy, disrupting farming activities and markets, particularly in rural areas. Furthermore, the EVD devastated the health care system. At the Peripheral Health Units (PHUs) that provided a basic package of essential health and nutrition services, fear of EVD infection by both health care professionals and community members rendered many PHUs non-functioning during the peak of the crisis. The loss of significant number of health care professionals contributed to a reduced confidence in the health care system. Traditional practices, including burial rites, were banned as a means of preventing Ebola transmission.
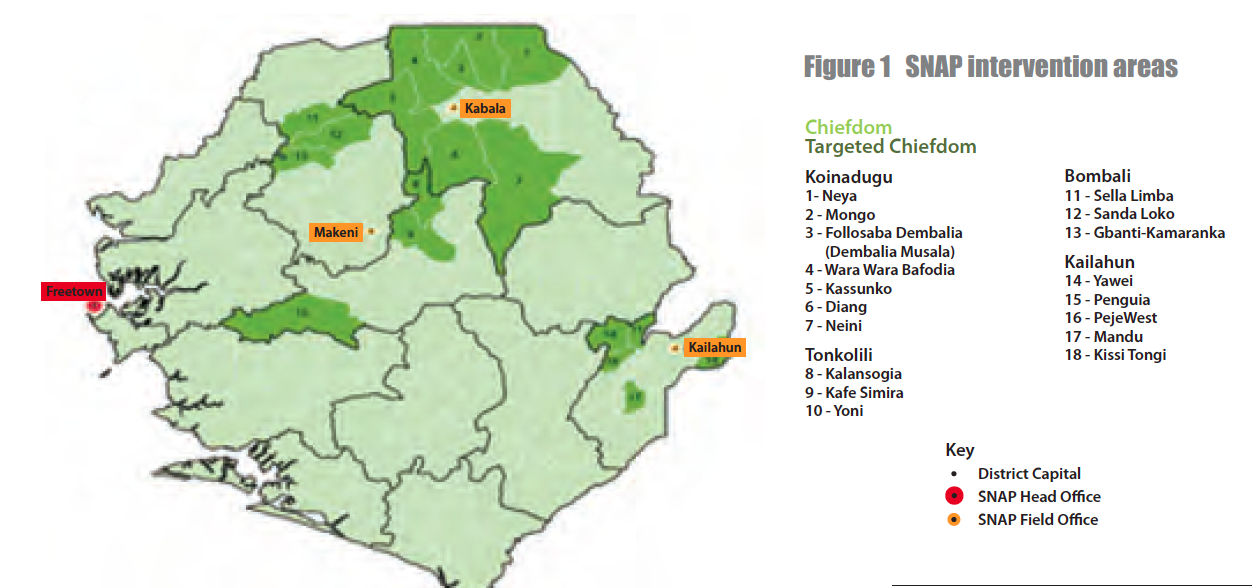
The Sustainable Nutrition and Agriculture Promotion (SNAP) programme is a multi-year assistance programme (MYAP) supported by USAID and has been implemented in four districts (Kailahun, Koinadugu, Bombali and Tonkolili) of Sierra Leone since June 2010. The goal is to reduce food insecurity and increase resilience among vulnerable rural populations in target districts. The SNAP programme has two strategic objectives: (i) reduce chronic malnutrition among children under-fives and (ii) enhance livelihoods for vulnerable people, especially women and youth. SNAP intervention areas are outlined in Figure 1 (see map).
The SNAP programme is implemented by a consortium of three partners:
- ACDI/VOCA is the primary partner engaged in agricultural livelihoods, village savings & loans associations, direct distribution activities and monetization, and gender mainstreaming.
- International Medical Corps (IMC) provides health, nutrition and WASH services including integrated management of acute malnutrition (IMAM); hygiene promotion at peripheral health units (PHUs) and communities; training and capacity building of health and nutrition service providers; and implementation of social and behavior change activities.
- Opportunities Industrialisation Centres International1 is engaged in youth livelihoods, literacy, numeracy and vocational trainings.
The Government of Sierra Leone (GoSL) Ministries involved in SNAP include Agriculture, Forestry & Food Security; Health & Sanitation; Finance & Economic Development; Social Welfare, Gender & Children’s Affairs and Youth Employment & Sports. The District Health Management Team (DHMT) is the focal point for SNAP at district level.
The EVD outbreak affected rural areas where the SNAP programme was being implemented. This article describes the SNAP programme prior to the outbreak, the changes that took place in response, and how the programme is transitioning back during recovery.
Programme approach and beneficiary targets prior to EVD outbreak (June 2010-May 2014)
In order to reduce chronic malnutrition (stunting) among children under-five, SNAP targeted 50,064 mother-child units through the ‘preventing malnutrition in children under two (PM2A)’ approach, specifically through the mother care group (MCG) model. A total of 350,448 household members were reached with health and nutrition messages/services in 18 chiefdoms in Bombali, Koinadugu, Tonkolili and Kailahun districts. The entry criterion for the programme is pregnancy, with graduation when the child reaches 24 months.
The MCG sessions were animated by Lead Mothers (LMs) with the SNAP programme supporting about 2000 LMs. Four modules were rolled out during the MCG sessions including: early initiation of, and exclusive breast feeding, appropriate complementary feeding, essential hygiene actions, and family planning. In conjunction with the LMs, a total of 615 men have been voluntarily promoting standard health seeking behaviours in their communities. A formalised approach for engaging men as partners, especially in promoting improved reproductive health and hygiene practices, has been initiated.
In order to enhance livelihoods for vulnerable people, especially women and youth, 45,377 individuals directly benefited from farm and non-farm training opportunities and Farmer Field Schools formed into clusters with links to value chains. Adult literacy/numeracy, vocational training, village savings and loans associations (VSLAs) were also part of the initiative to support livelihoods.
The nutrition component of the SNAP programme was carried out through the MCG which promoted optimal IYCF practices, essential hygiene and family planning. There was active screening and referrals of children with severe acute malnutrition (SAM) to the nearest outpatient therapeutic feeding programme run by the Ministry of Health/UNICEF. Training was conducted for DHMT staff on nutrition, health, and community integrated management of both neonatal and childhood illnesses (IMNCI) approaches. In addition, food aid distributions targeted pregnant and lactating women to prevent chronic malnutrition in children under 2 years. The monthly food distribution comprised a mother/child ration of vegetable oil, bulgur wheat, and lentils in the hunger/lean season, and corn soya blend (CSB), vegetable oil and lentils at other times.
Health activities involved promoting antenatal care (ANC), support to delivery at the health facility, prenatal care (PNC), information on sexual reproductive health rights (SRHR), and family planning. Construction of WASH facilities included installing hand washing stations, latrines, and incinerators for proper disposal of medical waste. Basic hand washing stations- tippy taps - were provided at household level. Agriculture/livelihoods involved support to farmer field schools, seed inputs and training in improved agronomic practices as well as access to credit through establishment of village savings and loan groups. Vocational skills support focused on literacy, numeracy and life skills for mothers/caregivers in the PM2A.
Revised programming due to EVD outbreak
The EVD outbreak started in Kailahun district, one of the SNAP operational districts and spread rapidly through the rest of the country. All of the SNAP intervention districts were badly hit by Ebola, including one operational chiefdom in Koinadugu, which was the last district that was affected. During the EVD outbreak (June – December 2014), new activities were implemented and existing activities adapted to support the emergency response and help SNAP beneficiaries recover from the shock of the EVD outbreak. Existing structures and staff, volunteers and community health workers, as well as village and WASH health committees, all worked to implement activities.
Due to the state of emergency and the ban on public gatherings, food distributions under the PM2A programme were stopped at the end of July 2014. Food aid commodities were redirected to provide food aid to quarantined households, an important component of stemming the spread of the virus.
One important development related to the integrated management of acute malnutrition (IMAM). A self-screening approach using mid upper arm circumference (MUAC) and EVD standard operating procedures was developed. The MUAC self-screening is done by each mother/caregiver for children 6 -59 months. SNAP supported training of LMs and cascaded the self-screening training to other mothers on the use of the MUAC tool. The LMs collected monthly nutritional data on children screened for reporting. Children identified as MAM or SAM were referred to the peripheral health units (PHUs) for verification and receipt of nutrition care/support. A balanced ration of food aid commodities were used to provide appropriate foods to address MAM.
Additional new/adapted activities included:
- Social Mobilisation: Community sensitisation was carried out using mobile teams and community radio. EVD WASH committees disseminated EVD prevention messages and actions to take if a suspected EVD case was found in a community.
- Provision of basic protective supplies to PHUs: chlorine, detergents, soap, buckets, hand sanitisers, disposable gloves etc. were provided.
- EVD contact tracing and active follow up. Training and support was provided to the DHMT for contact tracing data management and reporting.
- Psychological first aid training of staff and partners.
- Training of DHMT in nutrition, health, c- IMNCI approaches adapted in the Ebola context.
- Rehabilitation of WASH facilities at PHUs: hand washing, latrines, incinerators. This was rolled out before the EVD outbreak but was utilised greatly in preventing EVD infection.
- Food Aid to EVD quarantine homes (see above).
- MCG sessions focused on Module 3 ‘essential hygiene actions’, especially proper hand washing.
 Post EVD outbreak
Post EVD outbreak
Since January 2015, with the EVD outbreak under control and the number of new cases declining, the SNAP programme has entered into a recovery phase (see Figure 2). Activities to June 2016 have involved:
- A return to the spectrum of MCG activities, promoting IYCF, essential hygiene and family planning.
- Promoting the resumption and utilisation of PHU services (including antenatal and postnatal care) with support from lead mothers and men as partners.
- Nutrition self-screening (by mothers) of children (6-59 months) has continued using the MUAC tool and EVD standard operating procedures (SOPs). Referrals of MAM and SAM to PHUs for nutrition care services.
- Building capacity of WASH and village health committees to ensure that WASH facilities are functional at health facility and community levels.
- Village savings and loans maintained and proceeds shared (no new groups formed) to enable beneficiaries to buy food on local market.
- Development of culinary recipes for use in MCGs cooking demonstrations. The recipe book includes important complementary feeding and weaning foods recipes. The culinary recipe book will be used for MCG cooking demonstrations and cooking at household levels.
Discussion
The SNAP ‘development’ programme successfully adapted and harnessed capacity to respond to a challenging emergency context.
Extreme infection control measures gave rise to the ‘no touch’ policy in nutrition screening. Use of MUAC for nutrition self-screening and case identification of children 6-59 months by mothers/careers and supervised by LMs was instrumental in continuing community-based screening of children for MAM and SAM. Feedback from mothers and caregivers on using the MUAC tapes has been positive. Mothers/carers contribute to the measurement of nutrition status of their children and feel part of the decision making process surrounding their children’s health. The process developed is user friendly: illiterate mothers can effectively use the MUAC tapes and feel confident about translating the colours (green-normal, yellow- MAM, red – SAM) into their local language. LMs can effectively complete self-screening data collection tools, which makes monitoring of the entire process easier and can provide effective follow-up to ensure that children are getting proper nutrition and their health status is improving over time. Given the advantages, this innovation in self-screening will continue in the SNAP programme post-EVD outbreak.
Because of the EVD response, there is now increased awareness about hand washing and hygiene practices, especially using tippy taps at households and community levels. Tippy taps and or hand washing stations (veronica buckets) are readily available in public places and households for hand washing.
For more information, contact: Sibida George, email: sgeorge@internationalmedicalcorps.org
1http://www.oici.org