
Building the ‘enabling environment’ via a multi-sector nutrition platform to scale up micronutrient supplementation
 By Paula Quigley, Emmanuel Sokpo and Kate Godden
By Paula Quigley, Emmanuel Sokpo and Kate Godden
Dr Paula Quigley is a public health professional with over 25 years of international experience in health programme design, management, implementation and evaluation. A Partner at Health Partners International (HPI), her experience includes reproductive, maternal, newborn and child health and nutrition; HIV/AIDS, malaria programme management; capacity-building and community mobilisation and empowerment.
Dr Emmanuel Sokpo is a specialist physician with extensive training in health policy, planning and management and wide knowledge, skills and experience in health governance. Currently a Partner at HPI consulting on health system strengthening in Nigeria and South Sudan, he also is the technical lead on the Zinc/L-ORS and Iron and Folic Acid Supplements (ZIFAS) project.
Kate Godden is the Principal Nutrition Adviser for HPI and works on the MQSUN project that provides technical assistance to countries which are scaling up their nutrition activities. She is a registered nutritionist with over 20 years experience in programme design, management, implementation and evaluation covering nutrition and food security.
The authors acknowledge DFID/UK Aid Match as funders of the Partnership for Reviving Routine Immunisation in Northern Nigeria/Maternal Newborn Child Health programme (PRRINN-MNCH), and the Micronutrient Initiative (MI) as funder with technical assistance support to the ZIFAS programme.
Location: Northern Nigeria
What we know: Maternal anaemia increases maternal and infant morbidity and mortality. Zinc supplementation improves diarrhoea management outcomes. Northern Nigeria is a particularly challenging context to achieve coverage of key nutrition interventions such as micronutrient supplementation.
What this article adds: The ZIFAS multi-sectoral project (2012-2015) combines efforts in health systems strengthening (HSS), including commodity procurement and supply chain management, women’s empowerment, and governance to provide a platform for improvements in nutrition. It built upon the earlier successes of a strong Immunisation/Maternal Newborn and Child Health programme in northern Nigeria. Achievements include increased coverage and utilisation of antenatal iron and folic acid supplementation (IFAS), improved health workers’ awareness of zinc and L-ORS in diarrhoea management, zero stockouts of commodities at health centres, and costed, integrated health plans that include IFAS. It has proved an efficient and feasible approach at scale in a challenging context.
Background
 Northern Nigeria presents some of the greatest challenges globally in providing adequate healthcare to its population and has extremely poor health indicators that are consistently worse than the rest of Nigeria (NPC, ICF, 2014). Nutritional indicators are equally worrying, with all northern states performing worse than their southern counterparts. Jigawa and Katsina have the highest prevalence of acute malnutrition in the country: in Jigawa, the prevalence of stunting in children under five is 59% and that of wasting is 17%; in Katsina, these figures are 58.5% and 24% respectively; in Zamfara, they are 56% and 16%; and in Yobe, 49% and 24%. In contrast, the figures for Lagos are 17% for stunting and 11% for wasting. On average, 61% of pregnant women in Nigeria receive antenatal care (ANC) from a skilled provider; in Katsina and Zamfara States, only 22% do so. Likewise, the North East and North West zones have the lowest levels of children with diarrhoea who are given oral rehydration therapy (ORT) or increased fluids.
Northern Nigeria presents some of the greatest challenges globally in providing adequate healthcare to its population and has extremely poor health indicators that are consistently worse than the rest of Nigeria (NPC, ICF, 2014). Nutritional indicators are equally worrying, with all northern states performing worse than their southern counterparts. Jigawa and Katsina have the highest prevalence of acute malnutrition in the country: in Jigawa, the prevalence of stunting in children under five is 59% and that of wasting is 17%; in Katsina, these figures are 58.5% and 24% respectively; in Zamfara, they are 56% and 16%; and in Yobe, 49% and 24%. In contrast, the figures for Lagos are 17% for stunting and 11% for wasting. On average, 61% of pregnant women in Nigeria receive antenatal care (ANC) from a skilled provider; in Katsina and Zamfara States, only 22% do so. Likewise, the North East and North West zones have the lowest levels of children with diarrhoea who are given oral rehydration therapy (ORT) or increased fluids.
In order to help address this situation, a three-year project, ZIFAS, led by HPI in consortium with NPHD Ltd, a Nigerian consultancy, and funded by the MI (March 2013-April 2015; £1.25m) was implemented between 1 December 2012 and the end of March 2015. It built on earlier successes in northern Nigeria achieved by the PRRINN-MNCH, which combined HSS with routine immunisation and maternal, newborn and child health interventions. PRRINN-MNCH was managed by a consortium of HPI, Save the Children and GRID Consulting, and was funded by UK aid from the UK Government (2006-2014; £68.5m). It achieved dramatic reductions in child mortality rates and large increases in immunisation coverage. The achievements from the PRRINN-MNCH provided an anchor for launching and scaling up additional nutrition-specific interventions.
ZIFAS is a multi-sectoral intervention that combines efforts in HSS, women’s empowerment, and governance to provide a platform for improvements in nutrition. ZIFAS is developing innovative strategies to improve upon the existing low coverage of low-osmolarity oral rehydration salts (L-ORS), zinc, and iron and folic acid supplements in the four states of Jigawa, Katsina, Zamfara and Yobe. ZIFAS focuses on increasing the coverage and quality of ANC using low-dose IFAS to reduce illnesses and deaths resulting from anaemia in pregnancy. It is also improving the quality of diarrhoea treatment and prevention in children under five using zinc, L-ORS and other preventive strategies. The importance of such forms of micronutrient supplementation is well established in the academic literature (Lancet 2008, 2013) and recommended in the Framework for Action from the International Conference on Nutrition (ICN2) held in November, 2014 (ICN, 2014).
HPI is coordinating inputs to achieve the following project objectives:
- Achieve and sustain coverage for diarrhoea treatment in children under five with zinc and L-ORS in the target states;
- Ensure sustainable supply of zinc, L-ORS and IFAS in public health facilities in the target states for the duration of the contract and beyond it;
- Strengthen the public health system in provision and monitoring of zinc and L-ORS for treatment of diarrhoea in children under five;
- Improve access to diarrhoea treatment for children under five through outreach activities;
- Increase and sustain the proportion of pregnant women who consume sufficient amounts of IFAS during pregnancy; and
- Stimulate demand from the community for services through Social and Behavioural Change Communication (SBCC), including community engagement to enhance early ANC attendance and early presentation for treatment of diarrhoea in children under five.
An innovative policy framework coupled with supply and demand side interventions was introduced to promote the use of zinc and L-ORS to treat diarrhoea in children and daily low-dose IFAS for pregnant women. As well as managing the ZIFAS programme, HPI enhances the enabling environment for nutrition action in areas such as improving service delivery systems, governance, community engagement in health and financing through:
- Integration of funding into public sector budgeting processes, thus laying the foundation for future funding from domestic sources, including the establishment of basket funds to enhance sustainability. (Basket funds are pooled funds from various public health sector partners and other sources with a clear management structure where transparent, joint decisions are taken on priorities for funding, thus enhancing accountability and drive for results.);
- High-level health policy dialogue strategy development and planning;
- Supporting government to develop legislation and regulation to guide policy implementation;
- Establishing platforms for donor coordination, harmonisation and resource mobilisation;
- Capacity-building of government partners on leadership, governance and service delivery for sustainable impact.
- Simplifying existing monitoring and evaluation (M&E) systems in the health sector using District Health Information System (DHIS) technology for collective action;
- Improving quality of care, including training of health workers and strengthening quality improvement processes in health facilities;
- Increasing demand for and equitable access to health services by building community knowledge and capacity to identify and put in place community systems to tackle key barriers to access to health. Examples of this include increasing the number of women who have standing permission to attend a health facility in the absence of a male companion; developing the skills of community volunteers to reach the most excluded and vulnerable families; and establishing community support systems such as mothers’ helpers and community funds.
Cross-sector implementation in ZIFAS
HSS efforts
 Using an HSS approach, ZIFAS seeks to ensure long-term sustainable supply of essential commodities in the public health system. This includes improving systems for forecasting and procurement as well as supply chain management, capacity-building for health managers and service providers, and strengthening government systems for policy, planning, budgeting and coordinated implementation, as well as joint M&E. The platform for HSS interventions was developed during the PRRINN-MNCH programme, which supported the principle of one health plan and budget, one implementation and one monitoring and review process, and strengthened health workforce capacity, planning and management, drug procurement and supply chain management, service delivery and health governance.
Using an HSS approach, ZIFAS seeks to ensure long-term sustainable supply of essential commodities in the public health system. This includes improving systems for forecasting and procurement as well as supply chain management, capacity-building for health managers and service providers, and strengthening government systems for policy, planning, budgeting and coordinated implementation, as well as joint M&E. The platform for HSS interventions was developed during the PRRINN-MNCH programme, which supported the principle of one health plan and budget, one implementation and one monitoring and review process, and strengthened health workforce capacity, planning and management, drug procurement and supply chain management, service delivery and health governance.
Having reliable data is essential for appropriate decision-making in the health sector and routine health information systems were strengthened in Nigeria under the Partnership for Transforming Health Systems (PATHS1) programme in 2002, using the DHIS. The DHIS is free and open-source software that is used in many countries in Africa, such as Ethiopia, Botswana, Tanzania, Zambia, South Africa and Nigeria. The upgraded DHIS2 is a web-based data management tool that provides a comprehensive system for capturing complete, correct and consistent data at all levels, in both online and offline modes. Information can be accessed from any location with a computer and an internet connection. DHIS2 has revolutionised access to Health Management Information System (HMIS) not just in the northern states, but across Nigeria, allowing real-time information to influence decision-making. Mobile phones are changing the way health workers are recording essential data. PRRINN-MNCH tested user-friendly mobile phone applications linked to the DHIS2 and achieved impressive improvements in data completeness and timeliness at relatively low cost. ZIFAS has been able to benefit from this platform to further strengthen health facility attendance data availability, which has helped in tracking coverage of implementation and monitoring of required indicators.
Commodity procurement and supply chain management
Although states have procurement policies, their experience in responding to market situational changes is ad hoc in nature. The common procurement challenges across all the states include the absence of formal annual procurement and distribution plans; the lack of procurement skills by staff; and the absence of reliable drug quantification data. The ZIFAS project built on the PRRINN-MNCH platform to establish a harmonised system on the supply chain management system of ZIFAS commodities with other drugs, in line with the medium-term procurement and distribution guidelines, produced by ZIFAS. This collaborative effort was supported by other organisations such as UNICEF to strengthen the integrated management of ZIFAS commodities within the public health sector by providing more reliable data for an effective drug supply chain management system.
Women’s empowerment
Improving access to MNCH services in rural northern Nigeria requires a strategy that addresses all household and community barriers simultaneously and systematically. ZIFAS was able to build on achievements of several other programmes in the region, including PRRINN-MNCH, which works with isolated young women and their communities to improve their knowledge of MNCH issues and increase their access to key services. These successes were largely achieved through the efforts of community volunteers, many of whom were women themselves and who, as working women, also experienced a significant degree of empowerment from new-found respect within their communities. Volunteering is a valuable asset, putting local knowledge, skills, dynamism, creativity and concern for others to good use. Well-designed and managed community volunteer programmes can be effective and sustainable, with benefits beyond the health sector. The concept of a ‘community health team’ to complement health services and medically trained health providers is gaining traction in northern Nigeria.
Religious leaders play an important role in disseminating MNCH information across a large population and persuading communities to change established behaviour and attitudes. They can also help to promote a shift in thinking away from ‘charity’ towards broader-based support for those who are likely to suffer the heaviest burden of ill health. We found that a facilitative approach is required, wherein religious leaders are supported to use health-related information to devise their own key messages and preferred means of communicating them. ZIFAS is now able to build on this and promote nutrition-related messaging through community leaders.
Governance
The fragmented nature of healthcare delivery in northern Nigeria often results in intermittent programmes that are narrow in focus and limited in duration. State-wide health and coordinated planning has led to improved leveraging of extra resources that can be used more effectively. The extra resources, and their better use, led to health improvements in all four PRRINN-MNCH states and this now benefits ZIFAS. This sector-wide approach to health service provision can offer a variety of benefits to both governments and development partners and strong advocacy was used to ensure that the integrated health plans of each state included ZIFAS activities. The Primary Health Care Under One Roof strategy is another approach that was used by PRRINN-MNCH to bring together, through a legal framework, all the government health institutions and actors under one management and one authority to jointly manage health resources – money, manpower and materials – for the implementation of health interventions and to account for health outcomes. This framework was used by ZIFAS in mainstreaming its interventions into the state health sector; for improving the voice on nutrition-related issues; and enhancing the effective deployment of ZIFAS resources for greater value-for-money.
Results
Impressive results were achieved by PRRINN-MNCH in a highly challenging operational environment exacerbated by security concerns, including:
- Infant mortality reduction of 44% (from 90/1,000 live births to 51);
- Under-five mortality reduction of 41% (from 160/1,000 live births to 95); and
- Maternal mortality reduction of 6% (from 1,271/100,000 live births to 1190).
Contributing to these outcomes and a key result of these complementary areas of support was improved availability and quality of ANC, with the average proportion of women receiving ANC by a skilled healthcare worker doubling from 25% to 51% in the four states between 2009 and 2013. Women delivering their babies by skilled birth attendants increased from 11% to 27%. Women attending ANC with trained health care providers are more likely to receive nutrition advice, multiple micronutrient supplementation and malaria prevention, which all reduce the risk of maternal death and having babies with low birth weight (Lancet Nutrition Series, 2013). Those delivering with skilled birth attendants (SBA) are also more likely to start early breastfeeding and know about danger signs for themselves and their babies. Thus, PRRINN-MNCH was already implementing a nutrition-sensitive approach.
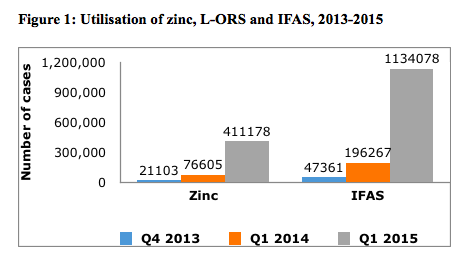
These successes have laid a strong foundation for ZIFAS and other programmes and initiatives to build on and expand and have enabled ZIFAS to reach more women from the start of the programme and achieve faster results. Likewise, the increased access of children to essential child health services has allowed ZIFAS to scale up improved treatment of diarrhoea with zinc and L-ORS. ZIFAS has resulted in increased outcome indicators for coverage and utilisation of low-dose IFAS for ANC and has improved IFAS commodity distribution and availability to over 1,000 health facilities (see Figure 1) in four states covering a population of approximately 19 million. Further achievements to date for nutrition from the ZIFAS programme include:
- Through the UN Population Fund (UNFPA), 93 million IFAS tablets have been procured and distributed to the health centres in the four states to meet a two-year need of these states.
- Costed, integrated health plans that include ZIFAS activities have been produced in the targeted states;
- Medium-term procurement and distribution plans and stock management tools have been developed;
- The existing HMIS is used to track key project indicators;
- Percentage of girls and boys with diarrhoea whose treatment included zinc and L-ORS in the recommended dose increased from a low level of 4.2% up to 54.5%;
- Percentage of frontline health workers aware of the need to use zinc and L-ORS in treatment of diarrhoea rose from 9% at baseline to 100% at the end of the project;
- Percentage of LGAs with zero stockout of ZIFAS commodities increased from 0% at baseline to 100% at the end of the project.
- All community engagement sites in the four states are fully mobilised and SBCC materials have been used (fact sheets, posters and TV/radio jingles).
- Advanced progress has been made in collaboration with the Federal Ministry of Health and other partners towards revising the national essential medicines list and standard treatment guidelines to incorporate low-dose IFAS.
Key lessons learned
ZIFAS uses an innovative, integrated approach that built on HSS achievements, an extensive community-engagement approach and stronger governance in northern Nigeria, which has facilitated significant scale-up of nutrition interventions. HSS measures, including health management information systems, have led to the improved use of commodities and better tracking of micronutrient supplements. This has resulted in increased outcome indicators for coverage and utilisation of low-dose IFAS for antenatal care and has significantly improved IFAS commodity distribution and availability.
 Successes have been achieved by working in innovative ways with government and communities to address political and social barriers at all levels, and thereby create an enabling environment. The community-engagement approach addresses all barriers faced by communities in accessing essential MNCH services, and builds social capital and cohesion to increase participation of the most marginalised families and reach those most at risk of ill health. The retention rate of volunteers was very high, indicating sustained commitment. The proportion of women with standing permission to take their child to a health centre when sick increased from 40% to 83%. In our approach, we work together with the Ministry of Women’s Affairs and Social Services, linking appropriate health-seeking behaviour to women’s empowerment, social protection, and safety nets through the community response systems supported and the inclusive approach taken to reach the most isolated and vulnerable families. Ensuring involvement of religious and community leaders, men, local government and other key stakeholders is an important way to build partnerships, promote mutual awareness of different perspectives, and increase accountability.
Successes have been achieved by working in innovative ways with government and communities to address political and social barriers at all levels, and thereby create an enabling environment. The community-engagement approach addresses all barriers faced by communities in accessing essential MNCH services, and builds social capital and cohesion to increase participation of the most marginalised families and reach those most at risk of ill health. The retention rate of volunteers was very high, indicating sustained commitment. The proportion of women with standing permission to take their child to a health centre when sick increased from 40% to 83%. In our approach, we work together with the Ministry of Women’s Affairs and Social Services, linking appropriate health-seeking behaviour to women’s empowerment, social protection, and safety nets through the community response systems supported and the inclusive approach taken to reach the most isolated and vulnerable families. Ensuring involvement of religious and community leaders, men, local government and other key stakeholders is an important way to build partnerships, promote mutual awareness of different perspectives, and increase accountability.
Conclusion
This type of comprehensive programming promotes efficiency through implementation of mutually beneficial interventions and a life-cycle approach to individuals and their health. PRRINN-MNCH delivered a range of outcomes at an estimated cost per person of £0.43 in 2013 (this equates to a cost of between £16 and £33 per child life saved). The programme’s comprehensive approach to health system strengthening contributed to positive changes in a challenging setting; this has enabled ZIFAS and other programmes to build on this foundation and achieve faster and more sustainable results. This approach strives to address inequity by eliminating a critical set of barriers to access; providing the local insight that can enable health workers and volunteers to address nutrition, health and social issues by close interaction with key stakeholders in their communities; and ensuring improved disaggregation and use of data to demonstrate coverage and progress of the project objectives.
For more information, email Dr. Paula Quigley
References
Demographic and Health Survey, (2013). Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International.
ICN, (2014). Access the Framework for Action and other key documents at www.fao.org/about/meetings/icn2/en/
The Lancet, (2008 and 2013). Maternal and Child Undernutrition Series. See www.thelancet.com/series/maternal-and-child-nutrition
National Population Commission (NPC) [Nigeria] and ICF International, (2014) Nigeria.