Community weighting of barriers and boosters in Democratic Republic of Congo
By Lenka Blanárová, Sophie Woodhead and Mark Myatt
Lenka Blanárová is a Community Mobilisation Advisor at ACF-UK, supporting nutrition programmes in Burkina Faso, Chad, Democratic Republic of Congo and Pakistan in the implementation of coverage assessments and the development of evidence-based community engagement strategies to boost their uptake and coverage.
Based within the ACF-UK Operations Team, Sophie Woodhead coordinates all activities and research projects under the Coverage Monitoring Network. She has supported a number of coverage trainings in west, east and central Africa as well as in Asia.
Mark Myatt is a consultant epidemiologist. His areas of expertise include surveillance of communicable diseases, epidemiology of communicable diseases, nutritional epidemiology, spatial epidemiology and survey design. He is currently based in the UK.
Location: Democratic Republic of the Congo
What we know: Perceptions of the relative importance of boosters and barriers to Community Management of Acute Malnutrition (CMAM) services access and coverage may differ between assessment teams and the community.
What this article adds: A recent case study examines the feasibility of involving community members in the weighting of barriers and boosters found using barriers-boosters-questions (BBQ) analyses in a SQUEAC assessment of programme coverage. Flash cards were used to present barriers and boosters to community members, followed by a ranking exercise and a weighting exercise (personal ballot of selected representatives and collective ranking). Weights were summarised for each barrier and booster using the median vote. Weightings given to barriers and boosters by the SQUEAC team and by community members did not always coincide; differences may not greatly affect the position of the prior mode but may, for example, influence programme reform. The method has potential but requires further development.
Introduction
Previous experience has shown that the Semi-Quantitative Evaluation of Access and Coverage (SQUEAC) assessment team’s perceptions of the relative importance of individual factors with a positive impact (boosters) and negative impact (barriers) on access and coverage may differ from the community’s assessment of the same factors. The input of community members is, therefore, potentially useful when weighting barriers and boosters for use in SQUEAC stage III assessments and for their translation into meaningful recommendations for programme reform. This case study examines the feasibility of involving community members in the weighting of barriers and boosters found using barriers-boosters-questions (BBQ) analyses in a SQUEAC assessment of programme coverage in Kirotshe health district, North Kivu Province, Democratic Republic of the Congo (DRC).
Methods and results
Following SQUEAC stage I qualitative data collection involving the daily organisation of barriers, boosters and questions using the BBQ tool, a small team of experienced SQUEAC assessment team members set out to test the feasibility of using community members to weight barriers and boosters. The work reported here took place in a single, purposively selected, exemplar community. The exemplar community was deemed to be broadly representative of the entire health district and chosen to be neither too close nor too far from the centre of the health district.
In preparation for the exercise, a set of large (i.e. A4 size) flashcards each depicting a single barrier or booster were prepared. Flashcards were put together electronically using copyright-free images available online. Figure 1 and Figure 2 show examples of flashcards for two barriers.
Multiple sets of voting cards displaying weights 1, 2, 3, 4, 5 and 6 were also prepared. These were designed and printed using different colours for each weight in order to facilitate the weighting process for participants with weak basic numeracy skills (see Figure 3).
The selected exemplar community was informed about the purpose and organisation of the exercise in advance and participation agreed. A group of five men and five women took part in the exercise. Only three persons of each sex voted.
Following an introduction, during which participants were encouraged to speak for the whole health district rather than focus on the needs of their own family or community, the team presented the identified barriers and boosters one by one using the set of flash cards and adding relevant descriptive and narrative detail gathered during stage I of the SQUEAC investigation.
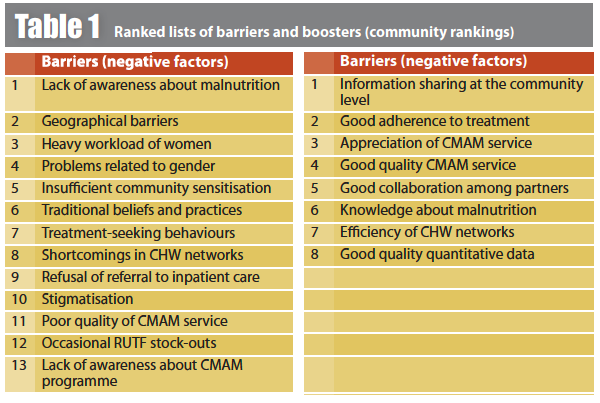
After each barrier and booster had been presented and explained, the relevant flash card was placed on the ground for all participants to see and ask questions (see Figure 4). When all uncertainties were clarified, participants were asked to discuss and rank barriers in order of importance, starting with those likely to have had the biggest impact on coverage and access to treatment. This exercise was repeated for boosters. Table 1 presents results of the ranking exercise for both barriers and boosters.
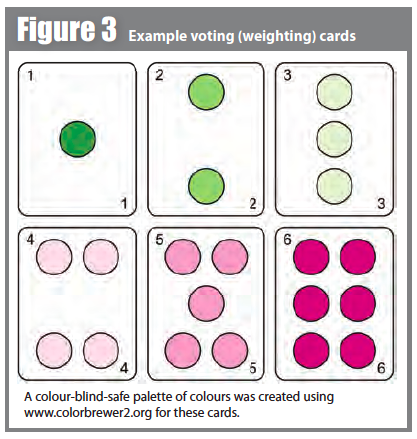
A colour-blind-safe palette of colours was created using colorbrewer2 for these cards.

Upon completion of the ranking exercise, the team explained the weighting exercise.
Three men and three women were selected and each received a complete set of voting cards (see Figure 3). The planned weights ranged between one (lowest impact on coverage) and six (highest impact on coverage). Given the large number of barriers and boosters identified during stage I of the SQUEAC investigation, it was decided that participants needed to vote on a scale ranged between one and seven. A weight of seven was achieved using two voting cards (e.g. a weight of seven was formed from 6 + 1 or 5 + 2 or 4 + 3).
When ready, participants were asked to turn their backs on the other participants in order to limit the influence on their voting. Women tended to shuffle voting cards under their garments to prevent others from peeking.
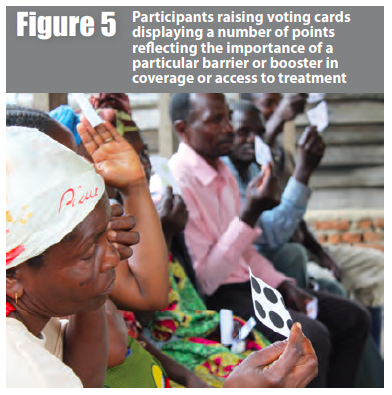
The team reviewed each barrier separately and participants voted by raising voting cards displaying a number of points reflecting the perceived importance of a particular barrier on coverage or access to treatment (see Figure 5). This process was repeated for boosters.
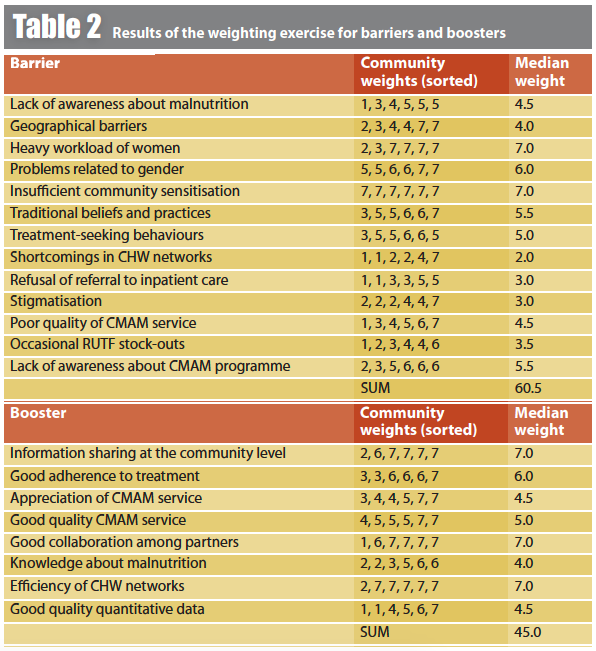
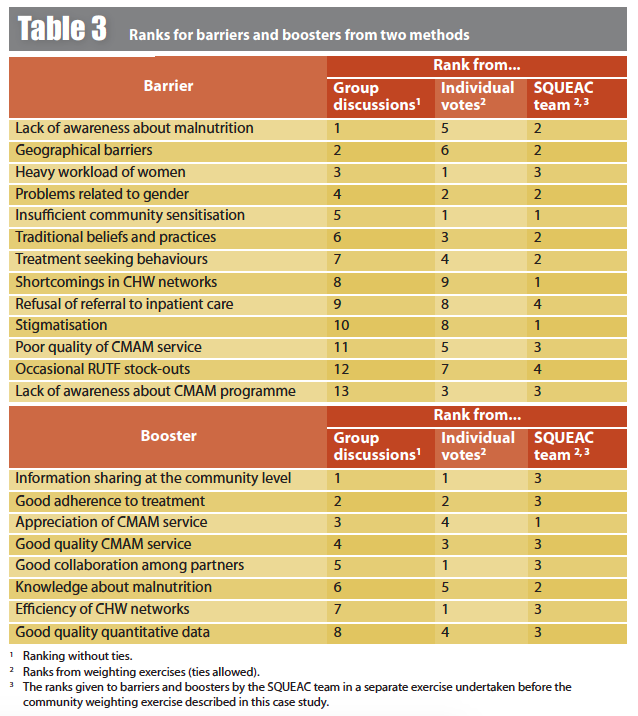
Table 2 shows the results of the weighting exercise for barriers and boosters. The weighting of barriers and boosters did not always coincide with their collective ranking or with the rankings of the SQUEAC team (see Table 3). The discrepancies between the collective ranks and the ranks from voting show that ‘consensus’ approaches may yield different results from ‘private ballot’ approaches and this can form the basis for further discussions with the group.
Results (i.e. Table 2 and Table 3) were presented to the group. Group members were invited to voice additional opinions and suggest recommendations for the improvement of the provided Community based Management of Acute Malnutrition (CMAM) services.
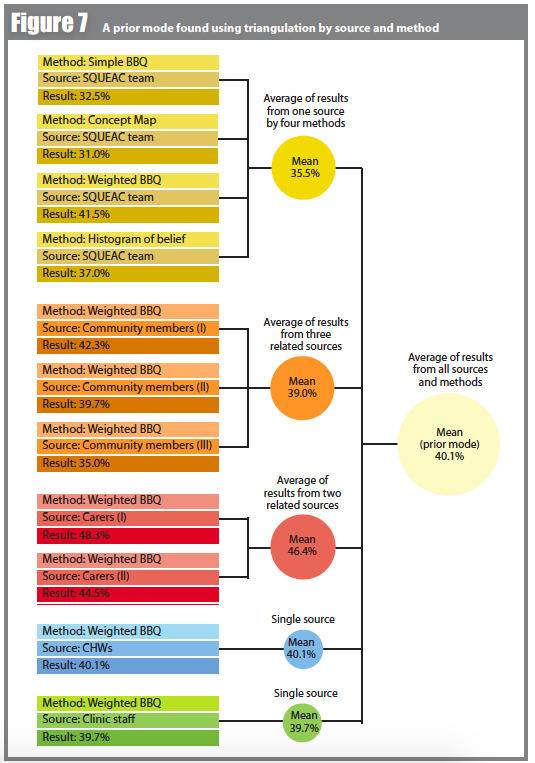
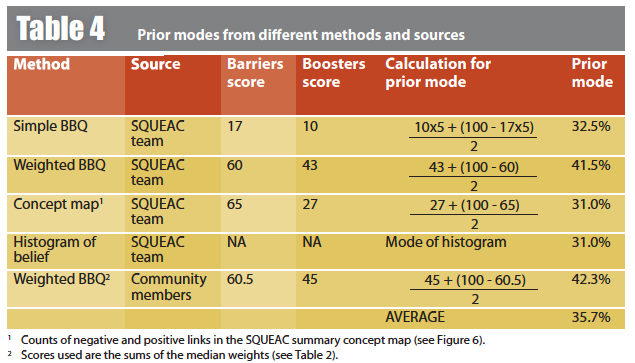
The ‘private ballot’ results were combined with other results from other sources and methods (i.e. using a simple average) to decide an appropriate prior mode for uses in the SQUEAC stage III survey (see Table 4).
Conclusions
The work presented in this case study demonstrates that it is feasible to use members of the community to weight barriers and boosters and provide input into the development of the prior for the SQUEAC stage III surveys. Such a prior would follow the SQUEAC principles of triangulation by source and method.
The finding that weightings given to barriers and boosters by the SQUEAC team and by community members did not always coincide suggests that the approach has value. Such differences may not greatly affect the position of the prior mode used in the SQUEAC stage III survey. In the work reported here, the position of the prior mode from the SQUEAC team alone (i.e. mean of the four methods used) was 34.0% and the position of the prior mode with community weighting added was 35.7%. The differences may, however, be useful to inform the priority given to different programme reforms. For example, the discrepancy between the SQUEAC team’s weightings and the community weightings with regard to the efficiency of the Community Health Worker (CHW) network found in the work reported here suggests that more data should be collected to inform reforms of the CHW network.
It is important to note that the work presented in this case study is not intended as a complete model of what should be done in SQUEAC assessments. If the community-weighting method is to be applied, it may prove useful to increase the range of sources used for community-based weighting to include, for example, all ethnic and religious groups, communities near to and distant from programme sites, community health workers/community-based volunteers, clinical and other programme staff and carers of children attending the program. The use of a diverse set of sources would follow the SQUEAC principle of triangulation by source.
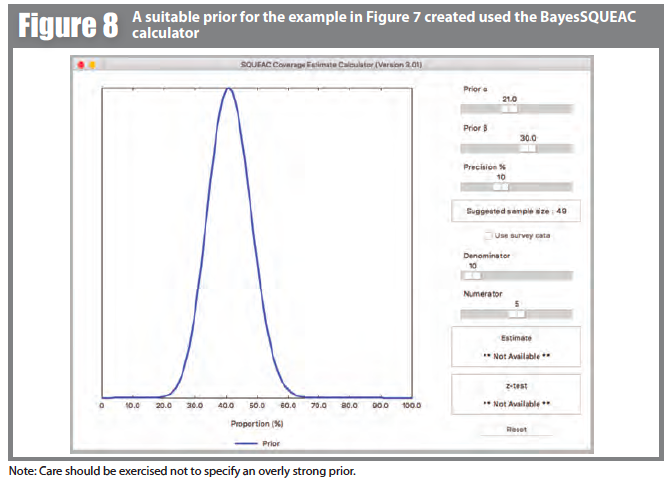
Combining results from different sources and methods could follow a hierarchical method in which the prior modes from related sources are averaged and then the prior modes from all sources are averaged. This process is outlined graphically in Figure 7. In the hypothetical example here, the prior mode is 40.1%. The width of the prior mode could be calculated as:

Figure 8 shows a suitable prior for the example shown in Figure 7 created with the BayesSQUEAC calculator. Care should be exercised not to specify an overly strong prior. It is probably not a good idea to specify a range narrower than ± 15%.
The work presented here shows promise. The method does, however, require further development before it can be recommended for use as a standard component of SQUEAC assessments.
Programme implementers and SQUEAC practitioners are encouraged to use community-feedback mechanisms (such as those described in this case study) in order to improve service delivery. These may be integrated into SQUEAC assessments or done as separate programme activities. Experiments, developments and findings could be submitted to Field Exchange for publication or presented and discussed on the en-net coverage assessment forum: www.en-net.org/forum/16.aspx.
For more information, contact: Sophie Woodhead