
Community-based management of severe malnutrition: SAM and SUW in children under five in the Melghat tribal area, central India
By Dr Vibhavari Dani, Dr Ashish Satav, Mrs Jayashri Pendharkar, Dr Kavita Satav, Dr Ajay Sadanshiv, Dr Ambadas S Adhav and Dr Bharat S Thakare
Dr. Vibhavari Dani is a pediatrician and Head of the Research Division, MAHAN (Meditation, AIDS, Health, De-Addiction, Nutrition), Melghat. She is the principal investigator of the study and helped in planning the research, monitoring and training staff and treatment of non-responding cases.
Dr. Ashish Satav is President of MAHAN, Melghat. He is co-Principal Investigator and helped in planning the research, monitoring and training of staff and arranging resources needed for the research.
Mrs. Jayashri Pendharkar works in the Department of Dietetics and is Nutrition Consultant and Treasurer at MAHAN, Melghat. She helped in planning therapeutic food dishes and training for the same.
Dr. Kavita Satav helped in mobilisation of resources, motivating co-Principal Investigators in starting the study and helping in recipe planning.
Dr. Ajay Sadanshiv is Chief Trainer and Chief Medical Officer with MAHAN.
Dr. Ambadas S Adhav is Project Manager. He helped in managing the project and regular monitoring.
Dr. Bharat S Thakare is Administrative Officer and Project Manager at MAHAN, Melghat. He helped in monitoring therapeutic food preparation, the calculation of nutritious food needed for RUTF and monitoring and cleaning data.
The authors would like to acknowledge caring friends in Mumbai for funding from Stichting Geron and Cordaid, Netherlands, guidance from Dr. Abhay Bang of SEARCH on the home-based child-care programme and Dr Raj Bhandari for his detailed review of this article.
Location: Melghat, India.
What we know: Severe acute malnutrition (SAM) and severe underweight (SUW) are prevalent among tribal community children in Melghat. Access to hospital-based treatment is limited; community-based treatment is not available.
What this article adds: A community-based prospective trial to treat SAM and SUW was conducted in tribal Melghat from August-October 2012, with six-month follow-up. A sample of 145 severely malnourished children (aged six to 60 months) was selected using a one-stage cluster sampling from 14 randomly chosen villages. Locally prepared therapeutic food (MAHAN-LTF) with micronutrients, infection treatment and behaviour-change communication were provided by Village Health Workers (VHWs) for 90 days. After eight weeks, 55.1% of SAM cases and 15.6% of SUW children had recovered. At 12 weeks, 63% of SAM and 28.7% of SUW cases had recovered. Case fatality rate for SAM was 2.0% and 0.8% for SUW. A recorded history of low birth weight (LBW) was found in 42.9% of SAM children and 46.9% of SUW children. The six-month relapse rates for recovered SAM and SUW were 3.03% and 11.1% respectively. Further research on community-based management of SUW is needed. This study will inform an ongoing randomised control trial on community-based management..
Introduction
Globally, malnutrition remains one of the leading causes of morbidity and mortality among children (Caulfield et al, 2005; Bhan et al, 2003; David, 1993), contributing to 60% of deaths in children aged under five (Caulfield et al, 2005; WHO, 1999). The prevalence of underweight children in India is among the highest in the world (for example, it is nearly double that of sub-Saharan Africa), with dire consequences for morbidity, mortality, productivity and economic growth (Gragnolati M, 2005). Prevalence of malnutrition among children remains alarmingly high in India, particularly among tribal populations. As per the National Nutrition Monitoring Bureau report 2009, the prevalence among one to five-year-olds is 6% for severe acute malnutrition (SAM), 20% for severe underweight (SUW) and 26% for severe stunting in tribal India (NNMB, 2009). Another study in tribal Maharashtra found prevalence of 7% SAM, 29% SUW and 30% severe stunting, considered ‘very high’ by WHO standards (Meshram et al, 2012; WHO Database). A study by the authors in 2012 showed very high (WHO Database) prevalence of severe malnutrition (7.1% SAM, 18.7% SUW, 34.4% severe stunting, and 6.7% grade III-IV malnourished (Indian Academy of Paediatrics (IAP)) in children under five years in Melghat (Daniet al, 2014). Major contributing factors for severe malnutrition are poor child-feeding practices, infectious disease, and poor hygiene and sanitation (Meshram et al, 2012; Amsalu et al, 2008; Bantamen et al, 2014). Co-existing infection increases risk of death among severely malnourished children (Ashworth, 2006).
Melghat is a difficult-to-reach, hilly, forest area in the state of Maharashtra, central India, with a population of 300,000 scattered over 320 villages, spread over 4,000 sq kms. Around 85% of the population is tribal, of whom more than 90% are small farmers or agricultural labourers living below the poverty line (Govt. of Maharashtra, 2009; MAHAN, unpublished). Medical facilities in the tribal area of Melghat are grossly inadequate and health-seeking behaviour is low (Satav et al, 2011; Govt. of Maharashtra; 2009). Hospital-based treatment is limited in coverage and impact. There is no specific programme to tackle this heavy burden of severe malnutrition in children aged six months to five years age and no community-based option. July to October is the period of heavy rainfall associated with a significant rise in infections, leading to increased malnutrition and child deaths within the year.
Given the above and the evidence around the community-based management of acute malnutrition approach (WHO/UNICEF/WFP/SCN, 2007; Manary et al, 2004; Schoonees et al, 2013), a one-stage, cluster randomised controlled trial for community-based management of severe malnutrition is underway, targeted at children aged six to 60 months in Melghat. It involved provision of local adapted therapeutic food (LTF) fortified with micronutrients, home-based treatment of infectious diseases and behaviour-change communication (BCC) delivered through village health workers (VHWs). Within this trial, a pilot study was conducted on community-based management and is described in this article.
Methods
This community-based prospective trial with one-stage cluster sampling method was conducted in the Dharni and Chikhaldara blocks in the tribal area of Melghat over a period of three months (August to October 2012). The sampling frame was all severely malnourished children (SMC) aged six to 60 months in 320 villages, from which 14 villages were randomly selected. The sample constituted 145 randomly selected target children from the usual resident population.
SAM was defined as weight-for-height Z scores (WHZ) ≤ 3SD with or without bilateral oedema. The presence of bilateral oedema was classified as SAM independent of WHZ. Underweight was defined as weight-for-age using WHO standardised Z scores (WAZ). SUW was defined as weight-for-age Z score (WAZ) ≤ 3SD (WHO, 2006). IAP gradations were defined as per percentage of expected weight for age: grade III: 50-60%, grade IV: <50% of expected weight (Achar, 1982). Customised software MAHANsoft version 1.0, 2011 was used for data entry and gradation purpose.
The project was implemented by the MAHAN (Meditation, AIDS, Health, De-Addiction, Nutrition) Trust, Melghat, in each village through semi-literate, tribal, local married women working as VHWs. One VHW per village was selected during Gram Sabhas (village meetings)1, which increased acceptance by the community. The villages have an average population of 900. VHWs were paid an honorarium as an incentive. They were trained on anthropometric assessment; feeding MAHAN-LTF with micronutrients (MAHAN-LTFMN, see Box 1); treatment of infectious diseases; and BCC through health education of parents. A total of 14 VHWs in 14 villages were involved.
Box 1: MAHAN-LTF with added micronutrients (MAHAN-LTFMN)
MAHAN-LTFMN is a local adaptation of the diet, prepared by local tribal women in the form of six palatable dishes (chivada, groundnut tilgul patti, dalia poha, moong dal khichri, groundnut sago, bhajani thalipeeth/upama). The therapeutic foods are prepared from ingredients such as groundnuts, oil, rice, sesame, jaggery, tapioca, gram dal, moong dal, etc. These ingredients are locally available, acceptable to the children, can be prepared by tribal women with minimum infrastructure, are palatable, and most have a shelf life of up to 21 days. Each 100g packet of MAHAN-LTFMN provides 500 to 550 kcals and around 15-17g of protein, according to the WHO formulation (WHO, 2007). Depending on the micronutrient deficit in each recipe, they were supplemented with micronutrients using a MAHAN VITAMIN mix powder produced by a pharmaceutical company.
Written informed consent was sought from the villagers during Gram Sabhas organised in each of the selected villages. The study received approval from the institutional ethical committee, which has six external members as per the recommendations of the Indian Council of Medical Research. The food material and associated set-up was approved by the Food and Drug Administration (FDA) of Amaravati.
In July 2012, anthropometry was measured in all targeted children by VHWs and cross-checked by medical supervisors (specially trained doctor and auxiliary nurse midwives (ANMs). Anthropometry included weight, measured by standardised Salter weighing machines, and height/length, recorded by standardised stadiometers.
Out of 145 study subjects, 59 were identified with SAM, 125 as SUW, 59 as IAP grade III-IV malnourished and 92 as severely stunted. Many children were suffering from acute-on-chronic malnutrition (SUW) and/or fell into more than one category of severe malnutrition. Parents of these severely malnourished children (SMC) were beneficiaries for BCC during the study period.
All identified severely malnourished children undertook an appetite test as per WHO guidelines (WHO, 2007). Children were screened for medical complications and those with serious illness were referred to hospital. Those who were not willing to go to hospital were managed by VHWs after providing high-risk written consent. Those who passed the appetite test were enrolled for 90 days of MAHAN-LTFMN therapy. If a child recovered before 90 days, they were still retained in the programme for the duration.
MAHAN-LTFMN was given to severely malnourished children four times a day under direct supervision of VHWs for 90 days. Children attended the house of the VHW for feeding observation; only in exceptional cases were cases fed at home (e.g. parents working away from home on a remote farm). Parents were asked not to give any other food during the course of therapy. According to the child’s weight, a specified amount of feed was provided so that all children received four to six grams of protein/kg/day and 175 kcal/kg/day, with gradual escalation. Anthropometry of enrolled children was monitored weekly for 12 weeks. Quality control of MAHAN-LTFMN involved random checking for accuracy of exact weight of each ingredient and hygiene. A taste register was maintained for any adverse reaction and palatability issues. At the outset, external quality control was undertaken by the District FDA Department.
The trained VHWs provided treatment for infectious diseases, such as fever, diarrhoea, acute respiratory infection (ARI), otitis media, malaria, deworming, etc. using paracetamol, norfloxacin, half-strength oral rehydration solution (ORS), amoxicillin, chloroquine and albendazole in appropriate doses (WHO, 2007). BCC of parents involved health education regarding hand-washing, nail-cutting, hygiene and nutrition through counselling, flipcharts, audio-visual film screening, practical demonstrations and street play. All activities were supervised weekly by medical supervisors and fortnightly by BCC supervisors.
Study limiting factors
Melghat is characterised by hilly, forest terrain with poor round-the-year availability of transportation and drivable roads. Annual rainfall is 1,500 mm and there are frequent flash floods. Heavy rainfall and floods led to interrupted supply of MAHAN-LTFMN to some villages. During the rainy season, it was difficult to maintain proper hygiene and sanitation at the storage and feeding sites of MAHAN-LTFMN in the villages. Although MAHAN-LTFMN preparations were made on the basis of socio-cultural habits and palatability, some of the preparations were not accepted by children and others had a lower shelf life than intended. As this was a new project, despite intensive training, VHWs and supervisors made mistakes in maintaining records. Weekly anthropometry records for a control group were not feasible, hence a randomised control trial was not possible.
Results
Table 1 shows the background characteristics of the 145 study subjects. The distribution of study subjects was SAM 40.7% (59), SUW 86.2% (125), and IAP grade III-IV malnourished 40.7% (59). Male and female distribution was almost equal in total number of severely malnourished children. SAM was seen in more than 57% children aged 6-<24 months, while SUW was seen in almost two-thirds of children in the 24-60 months age group. IAP grade III-IV was seen in more than three-quarters of children in the 24-60 months age group. Low birth weight (LBW) was found in 42.9% of SAM children and 46.9% of SUW children (as measured by VHWs and supervisors (Bhan et al, 2003)); 95% of these were full-term LBW. There were 15 cases of complicated severe malnutrition (10.3%), who were referred to hospital but refused.
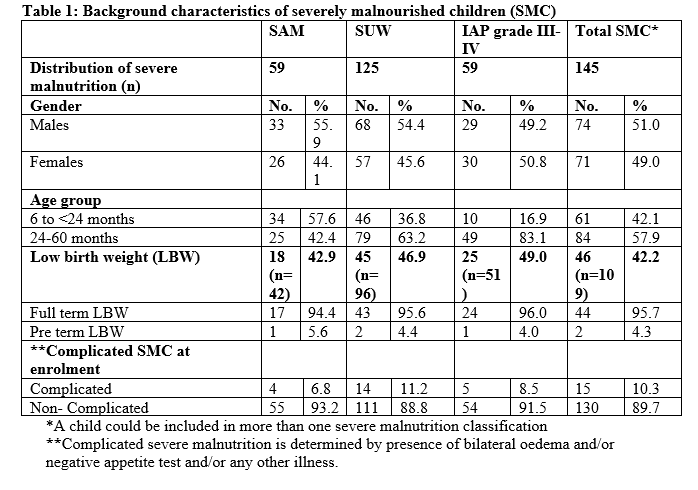
Table 2 shows recovery of severely malnourished child (SMC) and weight gain (g/kg/day) of recovered children at the end of the 8th, 10th and 12th week of MAHAN-LTFMN therapy. Recovery of SAM children was 55.1% at the end of eight weeks and 63% by the end of therapy. At the end of eight weeks, out of a total 49 enrolled SAM children, 27 (55.1%) recovered. At the end of 10th week, one recovered child dropped out, three recovered children relapsed and there was no new recovery. Thus, 23 (47.9%) out of 48 SAM remained recovered at the end of 10th week. At the end of the 12th week, out of seven dropouts, six were recovered children. Three children relapsed and four new children recovered. Thus, 18 (43.9%) out of 41 SAM remain recovered. In all, a total 31 children (63%) out of 49 SAMs were recovered by the end of therapy.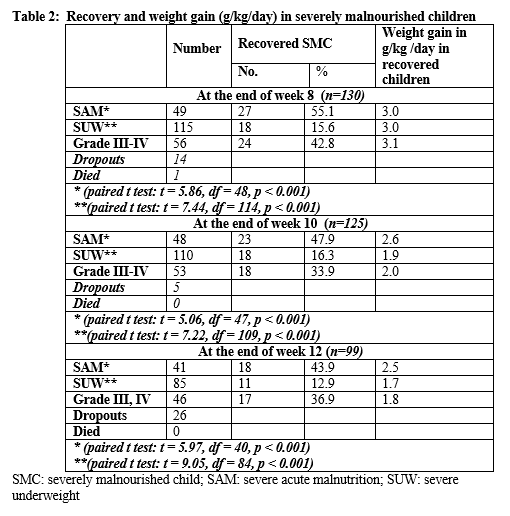
Recovery of SUW children is found to be 15.6% at the end of eight weeks and 28.7% by the end of therapy. At the end of eight weeks; out of a total 115 enrolled SUW children, 18 (15.6%) recovered. At the end of the 10th week, four out of five children that dropped out had recovered, five recovered children relapsed and nine children were newly recovered. Thus, 18 (16.3%) out of 110 SUW remained recovered at the end of 10th week. At the end of the 12th week, out of 25 dropouts, five were recovered children. Eight children relapsed and six new children recovered. Thus, 11 (12.9%) out of 85 SUW recovered. In all, total 33 children (28.7%) were recovered out of 115 SUWs by the end of therapy.
The children who relapsed during therapy did so either due to irregular attendance or episodes of infection. At the time of enrolment, there were 92 severely stunted children; none recovered by the end of therapy.
Paired t test for both SAM and SUW before and after the eight-week, ten-week and 12-week MAHAN-LTF intervention is significant (p<0.001).
Weight gain among SAM children after the 8th, 10th and 12th week was 3.0, 2.6 and 2.5 g/kg/d respectively; among SUW it was 3.0, 1.9 and 1.7 g/kg/d respectively. For IAP grade III-IV, weight gain was 3.1, 2.0 and 1.8 g/kg/d after the 8th, 10th and 12th week respectively. There were 14 dropouts and one death after eight weeks, five more dropouts after 10 weeks, and 26 more dropouts before completion of therapy. The case fatality rate (CFR) for treated SMC was 0.7%. The CFR was 1.7% for SAM, 0.8% for SUW and 1.7% for IAP grade III-IV.
Figure 1 shows the percentage weight gain in recovered SAM children (WHZ <-3 SD) after eight weeks of MAHAN-LTFMN. Recovery from SAM was seen in 27 (55.1%) out of 49 children. The percentage of weight gain among 17 cases (63.0%) of recovered SAM was <15%; for ten cases (37.0%) of recovered SAM it was ≥ 15%.
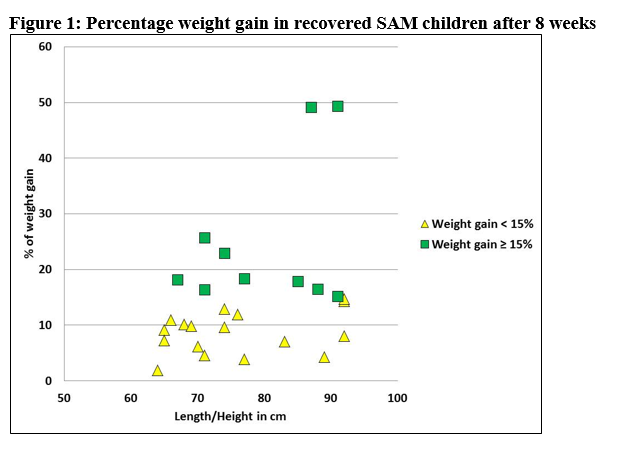
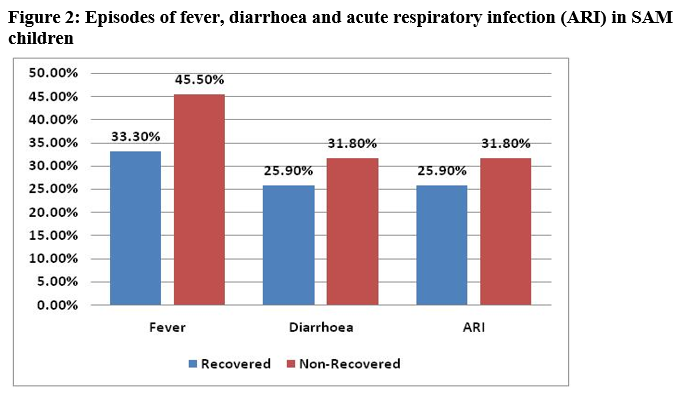
Figure 2 shows episodes of fever, diarrhoea and ARI in SAM children. A gap of seven days between two episodes was factored into data gathered. Non-recovered children had more episodes of infection.
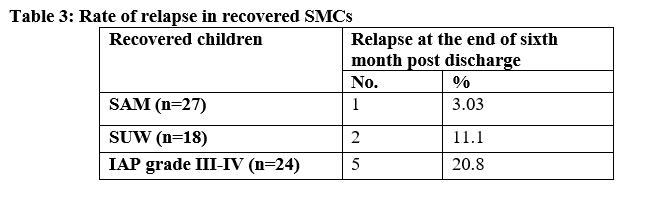
On discharge, all SMCs who had recovered at eight weeks were followed up for six months. Table 3 shows the rate of relapse in recovered SMCs. Of 27 recovered SAM children, one child (3.03%) relapsed; out of 18 recovered SUW children, two children (11.1%) relapsed, and out of 24 recovered IAP grade III-IV, five children (20.8%) relapsed.
Discussion
In our previous study, we had shown that the prevalence of SUW in the tribal community of Melghat is 18.7% and that of SAM is 7.1% (Dani et al, 2014). Co-existence of acute and chronic malnutrition needs to be comprehensively addressed with combined multiple approaches (Bergeron et al, 2012). It is therefore necessary to include SUW children, in addition to SAM cases, in a community-based therapeutic feeding project. We could not find any study on community-based management of SUW children. In this study, almost half of the SUWs were full-term LBW infants reflecting intra-uterine growth retardation; i.e. they were born malnourished.
Maternal and child health and nutrition services are required for prevention of chronic malnutrition. However, for management of severe, acute-on chronic malnutrition (SUW), our treatment regime of MAHAN-LTFMN achieved just 16.3% recovery. Relapse rate was greater among recovered SUW and IAP grade III-IV children compared to SAM children. It remains to be seen whether children with acute-on chronic malnutrition need longer follow-up, further investigations for chronic diseases and longer duration of therapy. A study published in 2001, based on the systematic review of studies published in the 1980s and 1990s, revealed that only six out of the 27 studies achieved case fatality rates of <5% and relapse/readmission rates of <10%, which can be taken as standard (Ashworth, 2001).
The duration of this pilot study was kept as 12 weeks and recovery from severe malnutrition at the end of the 8th, 10th and 12th week was assessed. We found maximum recovery and daily weight gain at the end of the 8th week. Over half (55.1%) SAM children recovered from severe malnutrition, with an average weight gain of 3.0 g/kg/day after eight weeks. The rate of weight gain decreased by the end of ten and 12 weeks of treatment. It is possible that rapid weight gain occurs when a child is wasted; as the child approaches a normal weight for height, the rate of weight gain falls (Ashworth, 2006). This fall in daily weight gain rate may reflect a greater proportion of defaulters as the duration of therapy lengthens.
Studies from India and elsewhere have discussed evidence-based possible interventions to address SAM, but the co-existence of acute and acute-on-chronic malnutrition in India cannot be denied and also needs to be addressed (NNMB, 2009; Meshram et al, 2012; WHO database; Dani et al, 2014). The preventive approach of addressing acute-on-chronic malnutrition will benefit future generations, but treatment is urgently needed for those who are already malnourished. The response to treatment demonstrated through this intervention is encouraging. More research needs to be done to determine the exact nature and duration of therapy for these children.
Weight gains up to 15% were seen in 63% of the recovered SAM children. Weight gain of 15% to 49% was seen in 37% of recovered SAM children; these children had good appetite, no episodes of infections, were non-defaulters and showed no relapse at the end of six months follow-up. Episodes of fever, diarrhoea and ARI were more common in non-recovered SAM children compared to recovered SAM. This indicates that timely treatment of infections in the community by trained VHWs will improve recovery rates and prevent relapse of severe malnutrition; it is important that a good referral system should be established.
Conclusions
Community-based management of severe malnutrition is possible and the treatment of SUW children has good potential. This pilot study is a part of a larger study which is underway with a sample size of 1,500 SMCs in each arm of an RCT. Such programmes lead to capacity-building of the community to deal with the menace of malnutrition. This study seems to demonstrate that this treatment approach is acceptable, cost-effective, achievable, safe and feasible with locally available manpower and resources.
For more information, Dr. Ashish Satav, email: drsatav@rediffmail.com; tel: +919423118877
References:
Achar 1982. The Classification by Nutrition Sub-committee of Indian Academy of Pediatrics. Report. Indian Pediatr 1972; 9: 360: and S.T. Achar, Textbook of pediatrics, 1982, 2nd ed. p. 252. ISBN-13: 978-0-86131-361-7
Amsalu S & Tigabu Z. Risk factors for severe acute malnutrition in children under the age of five: A case-control study. Ethiop J Health Dev. 2008; 22(1): 21-5.
Ashworth A. Efficacy and effectiveness of community-based treatment of severe malnutrition. Food and Nutrition Bulletin 2006; 27 (3): S20-S48
Ashworth A, Community-Based Rehabilitation of Severely Malnourished Children: a Review of Successful Programmes. London School of Hygiene and Tropical Medicine. Report. 2001.
Bantamen G, Belaynew W, Dube J. Assessment of Factors Associated with Malnutrition among Under Five Years Age Children at MachakelWoreda, Northwest Ethiopia: A Case Control Study. J Nutr Food Sci 2014; 4 (1): 256.
Bergeron G and Castleman T 2012. Responses to Acute and Chronic Malnutrition: Divergences and Convergences. AdvNutr March 2012 vol. 3: 242-249. http://advances.nutrition.org/content/3/2/242.full - aff-2
Bhan M, Bhandari N, Bahl R. Management of the severely malnourished child: perspective from developing countries. BMJ 2003; 326: 146-51.
Caulfield LE, de Onis M, Blossner M, Black RE. Undernutrition as an underlying cause of child deaths associated with diarrhoea, pneumonia, malaria, and measles. Am J Clin Nutr. 2004; 80:193–198
Dani V, Satav A, Pendharkar J, Ughade S, Jain D, Adhav A et al. Prevalence of undernutrition in under-five tribal children of Melghat: A community based cross sectional study in Central India, Clinical Epidemiology and Global Health 2014 Sept, I-8
David L. Epidemiologic Evidence for a Potentiating Effect of Malnutrition on Child Mortality. Am J Pub Health 1993; 83(8): 1130-3.
Govt. of Maharashtra. Human Development Indicators Among the Scheduled Tribes of Maharashtra. A Research Report by TRTI Pune. Government of Maharashtra; 2009. pp. 25 and 27 http://moef.nic.in/soer/state/SoE report of Maharashtra.pdf.
Gragnolati M, Shekar M, Das Gupta M, Bredenkamp C and Lee YK. India’s Undernourished Children: A Call for Reform and Action. Michele Gragnolati, Meera Shekar, Monica Das Gupta, Caryn Bredenkamp and Yi-Kyoung Lee. HNP Discussion Paper.
MAHAN Trust Report (unpublished).
Manary MJ, Ndekha MJ, Ashborn P, Maleta K, Briend A. Home based therapy for severe malnutrition with ready-to-use food. Arch Dis Child 2004-89: 557–561.
Meshram II, Arlappa N, Balakrishna N, Laxmaiah A, Rao MK, Reddy G et al. Prevalence and Determinants of Undernutrition and its Trends among Pre-School Tribal Children of Maharashtra State, India. J Trop Pediatr 2012; 58(2): 125-32.
NNMB Technical Report 25. Diet and Nutritional Status of Tribal Population and Prevalence of Hypertension among Adults. 2009.
Pelletier DL, Frongillo EA Jr, Schroeder DG, Habicht JP. The effects of malnutrition on child mortality in developing countries. Bull World Health Organ.1995;73(4):443-8.
Satav A, Sane BL, Bhapkar P, Shankarnarayan M, Parhi R, Bobde K et al, Counsellor Program for Saving Severely Malnourished Children by Improvement of Government Hospitals of Melghat : Result of a Field Trial. Pediatric Research (2011) 70, 828
Schoonees A, Lombard M, Musekiwa A, Nel E, Volmink J. Ready-to-use therapeutic food for home-based treatment of severe acute malnutrition in children from six months to five years of age. Cochrane Database Syst Rev. 2013; Jun 6
UNICEF 2005. The State of the World's Children: Childhood under threat. UNICEF Report http://www.unicef.org/publications/files/SOWC_2005_(English).pdf
WHO 1999. Management of Severe Under Nutrition, A Manual for Physicians and Other Health Workers. Geneva: WHO; 1999.
WHO 2006. Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: World Health Organization, 2006. www.who.int/childgrowth/standards/technical_report/en/
WHO Database. Global Database on Child Growth and Malnutrition – ‘Trigger-levels’ as a basis of public health decisions. www.who.int/nutgrowthdb/about/introduction/en/index5.html..
WHO/UNICEF/WFP/SCN Joint statement. Community-based management of severe malnutrition. Geneva, New York, Rome, 2007. www.who.int/child_adoloscent_health/documents/pdfs/severe_acute_malnutrition_en.pdf
1The Gram Sabha is the foundation of the Panchayati Raj system and formal unit of local government.