
Chronic disease outcomes after SAM in Malawian children (ChroSAM): A cohort study
Summary of research*
Location: Malawi
What we know: Little is known about the long-term health effects of survivors of severe acute malnutrition (SAM), particularly risk of non-communicable diseases (NCDs) in later life.
What this article adds: A cohort of Malawian SAM-survivor children were followed up seven years after inpatient SAM treatment and compared with sibling and community controls. Seven years post-treatment, nearly one-third of discharged cases had died and another 15% were lost to follow-up. SAM survivors had lower height-for-age (HAZ) compared with controls, although with evidence of catch-up growth. Associated functional impairments were found, such as poorer physical strength, poorer physical capacity, and lower school achievement, compared to controls. Results suggest that SAM has long-term adverse effects (patterns of growth associated with future NCDs), but with potential for rehabilitation (evidence of catch-up growth and largely preserved lung and cardiometabolic functions). Recommendations for future follow-ups include establishing the effects of puberty and later dietary or social transitions.
Extensive research links nutrition in early life with adult health and non-communicable diseases (NCDs), a field of research known as developmental origins of health and disease (DOHaD). Most evidence for DOHaD describes associations between in utero or very early postnatal exposures and adult NCD risk. However, it is biologically plausible that early life events such as severe acute malnutrition (SAM) during late infancy or early childhood, and the rapid catch-up growth that occurs during and after treatment, could have long-term health implications.
The chronic disease outcomes after SAM in Malawian children (ChroSAM) study followed up children seven years after they had received SAM inpatient treatment. Researchers investigated the effects of SAM on growth, body composition, functional outcomes and risk factors for NCDs.
Study overview
The original prospective cohort comprised 1,024 patients admitted for SAM treatment at Queen Elizabeth Hospital in Blantyre, Malawi, during a nine-month period (July 2006 to March 2007). All patients were treated with initial inpatient stabilisation using therapeutic milk, followed by nutritional rehabilitation with ready-to-use therapeutic food (RUTF) at home. The median age at admission was 24 months. The ChroSAM study group was made up of 320 surviving children from the original cohort, identified from a one-year post-discharge follow-up study (n=477). For comparison, the researchers aimed to recruit one sibling control (the sibling closest in age to the case child) and one community control (a child of the same sex and close in age living in the same community) per child in the case group. Children who had been treated for SAM were not eligible as controls.
The study’s outcomes of interest included: anthropometry, body composition, lung function, physical capacity (measured as handgrip strength, step test and physical activity), school achievement and blood markers of NCD risk. Multivariate linear regression was used to compare all outcomes, adjusted for age, sex, HIV status and socioeconomic status, as well as puberty in the body composition regression model. Data collectors were not blinded to the case or control status of the children. With 320 cases, 217 sibling controls and 184 community controls, the authors calculated that the study was adequately powered (at least 90% to detect a Z score difference of 0.5 between the cases and controls based on reference data for growth and lung function outcome). The sample size was considered adequate for all outcomes except physical activity (steps per day), which was underpowered.
Results
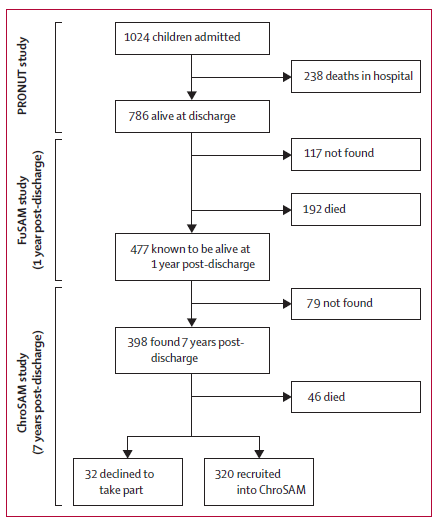
Of the 1,024 children originally admitted, 238 (23%) died during treatment. At one-year follow-up, 24% of children were known to have died (192/786 of those discharged); an additional 117 were lost to follow-up. Of 398 children traced seven years post-discharge, 46 (11.5%) had died. Thus, of 786 children discharged from SAM treatment, nearly one-third (30%) were known to have died seven years later and another 15% were lost to follow-up. (See Figure 1.)
Figure 1: Recruitment of the case group1
Key findings show:
- Case children had more severe stunting than controls (adjusted diference vs community controls 0·4, 95% CI 0·6 to 0·2, p=0·001; adjusted diference vs sibling controls 0·2, 0·0 to 0·4, p=0·04), although they showed evidence of catch-up growth.
- These children also had shorter leg length ((adjusted diference vs community controls 2·0 cm, 1·0 to 3·0, p<0·0001; adjusted di?erence vs sibling controls 1·4 cm, 0·5 to 2·3, p=0·002), but similar sitting height.
- Cases had other body composition differences than controls, including: smaller mid-upper arm circumferences (MUAC) (adjusted di?erence vs community controls 5·6 mm, 1·9 to 9·4, p=0·001; adjusted diference vs sibling controls 5·7 mm, 2·3 to 9·1, p=0·02); smaller calf circumference (adjusted diference vs community controls 0·49 cm, 0·1 to 0·9, p=0·01; adjusted diference vs sibling controls 0·62 cm, 0·2 to 1·0, p=0·001); smaller hip circumference (adjusted diference vs community controls 1·56 cm, 0·5 to 2·7, p=0·01; adjusted di?erence vs sibling controls 1·83 cm, 0·8 to 2·8, p<0·0001); and less lean mass (adjusted diference vs community controls –24·5, –43 to –5·5, p=0·01; adjusted diference vs sibling controls –11·5, –29 to –6, p=0·19).
- Survivors of SAM had functional deficits such as weaker handgrip (adjusted diference vs community controls –1·7 kg, 95% CI –2·4 to –0·9, p<0·0001; adjusted diference vs sibling controls 1·01 kg, 0·3 to 1·7, p=0·005), and fewer minutes completed of an exercise test (sibling odds ratio [OR] 1·59, 95% CI 1·0 to 2·5, p=0·04; community OR 1·59, 95% CI 1·0 to 2·5, p=0·05).
- Community and sibling controls were more likely to be in a higher school grade after adjusting for confounders (odds ratio [OR] 1·70, 95% CI 1·2–2·4, p=0·003 compared with community controls and OR 2·77, 95% CI 1·9–4·0, p<0·0001 compared with sibling controls).
Most of the other NCD risk factors assessed (such as lipid profle and glucose tolerance) were not significantly different between cases and controls, except for diastolic blood pressure, which was higher for cases than for sibling controls (adjusted diference 1·91 mm Hg, p=0·03). Amongst cases, 28% were confirmed HIV-positive (compared to 4% in sibling controls and 3% in community controls).
The authors identified a number of limitations to their research, including:
- Survivor bias, since only 352 out of 1,024 children in the original cohort were still alive for this follow-up (30 declined to take part); thus the study selected the fittest and healthiest survivors;
- Sibling and community controls are not fully healthy; and
- The study does not have data on potential confounders, such as exact birthweight and gestational age, which are linked to both SAM and long-term health effects.
Discussion
The results from the study suggest that SAM has long-term adverse effects, especially with regard to mortality, growth and body composition. SAM survivors continue to have signi?cantly more stunting than their siblings and other children in their community at seven years’ post-discharge from inpatient nutritional treatment. Associated functional impairments include poorer physical strength, poorer physical capacity, and lower school achievement than controls.
Despite greater stunting among cases, sitting height was similar to controls, suggesting that torso growth had been preserved while limb growth was compromised. Other outcomes such as head circumference were also similar in all groups, while lung function and HbA1c were close to normal when compared with children of African-American origin in all groups. This suggests that survivors of SAM might have undergone so-called brain-sparing or thrifty growth, whereby the growth of vital organs has been preserved at the cost of less vital growth.
Large sitting-to-standing height ratio, short limb length, lower peripheral mass, and larger waist-to-hip ratio have all been associated with NCDs in adulthood. The pattern of lower lean mass and preservation of fat mass seen in children in the case group is similar to that seen in children born with low birthweight (LBW). This is an important predictor of physical work capacity in later life. The combination of reduced lean mass and greater stunting compared with controls might explain the de?ciencies in physical function and strength seen in the SAM survivors. Weaker handgrip is also associated with lower bone mass, impaired cell membrane potential, and reduced muscle function, as well as all-cause early mortality, risk of malnutrition and risk of NCDs.
However, SAM survivors did show signs of growth recovery, with gain in HAZ increasing at a steeper rate in cases who were catching up to their sibling controls. The evidence for catch-up growth, as well as the apparent preservation of vital organs, suggests the potential for recovery following SAM. Yet case study children remain relatively small (compared with global population for this age), and organ damage might only become apparent when exposed to weight gain and unhealthy lifestyles (as seen in studies of LBW). SAM survivors may face potentially greater NCD risks due to changes in dietary trends in many African countries.
This study found high in-treatment and post-discharge mortality amongst children treated for SAM. The study period preceded the establishment of community-based management of acute malnutrition (CMAM) in Malawi with associated earlier detection of SAM and outpatient care options.
In conclusion, the study suggests that SAM has long-term adverse effects, with survivors showing patterns of ‘thrifty growth’ associated with future NCDs. Evidence for catch-up growth and preservation of vital organs suggests potential for rehabilitation, but future follow-ups need to focus on how to optimise recovery and minimise any long-term adverse outcomes.
*Lelijveld, Natasha, Andrew Seal, Jonathan C Wells, Jane Kirkby, Charles Opondo, Emmanuel Chimwezi, James Bunn, et al. 2016. “Chronic Disease Outcomes after Severe Acute Malnutrition in Malawian Children (ChroSAM): A Cohort Study.” The Lancet Global Health 4 (9) (September 14): e654–e662. doi:10.1016/S2214-109X(16)30133-4.
1 Flow diagram showing recruitment, starting with original recruitment in 2006 for the PRONUT study, followed by one-year follow up in the FuSAM study, and the present follow-up (ChroSAM).