 English
English Français
Français Deutsch
Deutsch Italiano
Italiano Español
Español
Pilot micronutrient powder distribution in Burundi: acting on lessons learned
By Leni Martinez Del Campo, Emily Sylvia and the Concern Burundi Team
Emily Sylvia is a recent graduate of the MPA in Development Practice programme at the Columbia University School of International and Public Affairs, where she specialised in agriculture and food security with a focus on nutrition-sensitive agriculture.
Leni Martinez del Campo was the food and nutrition security officer at Concern Worldwide, where she focused on advocating for greater political support and financial resources for nutrition. She is a graduate of the MPA in Development Practice programme at Columbia University.
The authors acknowledge the contribution of the Concern Burundi team to the development of this article and thank Kirk Pritchard of Concern for helping coordinate inputs.
Location: Burundi.
What we know: Micronutrient deficiencies are prevalent amongst children in Burundi. Micronutrient supplementation is one means of tackling it.
What this article adds: A pilot programme distributed a two-month supply of micronutrient powder (MNP) during Mother-Child Health Week, targeting children aged 6-23 months in two provinces of Burundi and supported by community health workers and peer educators. A post-distribution survey of mothers found high distribution coverage (97%), good acceptance of the product, and reported child health benefits (less sickness, more energy). Problems identified included inadequate community sensitisation and follow-up, mislabelled packaging (incorrect age group), and miscommunication between health workers and mothers. These likely affected uptake; 64% of mothers had not used all the supply by the end of the intervention period. Identified barriers were addressed to improve subsequent phases. This experience reinforces the importance of community engagement, feedback mechanisms and adaptive programming.
The current state of child nutrition in Burundi
In Burundi, four out of five people live on less than US$1.25 per day, making it one of the poorest countries in the world. It is also among the countries with the highest prevalence of stunted children: an estimated 58% of children under five years of age are stunted (height for age <-2 z scores). This is significantly higher compared to other countries in the East Africa region with similar per capita incomes.1 In addition, 35% of children are underweight and 7% are wasted.2 Less outwardly visible, micronutrient deficiencies are also prevalent. Twenty-five per cent of children under five years of age are vitamin A deficient and 56% are anaemic. Zinc deficiency affects 47% of the population.3 Adequate micronutrient intake is important throughout life, but critical during the first 1,000 days (from conception to second birthday) to ensure adequate cognitive and physical development. It is estimated that Burundi loses approximately US$30 million a year due to micronutrient deficiencies.4
MNP distribution project
In an effort to tackle micronutrient deficiencies within the 1,000-day window of opportunity, the Ministry of Public Health and the Fight Against AIDS of Burundi, in partnership with UNICEF, has undertaken widespread distribution of micronutrient powders (MNPs) for children aged 6-23 months as part of the Burundian National Integrated Program for Food and Nutrition (PRONIANUT). This article shares experiences from the pilot MNP distribution initiative in 2014 and 2015.
A pilot MNP distribution was carried out in December 2014 and April 2015 during Mother-Child Health Week (a twice-yearly event) in Cibitoke and Ngozi provinces. All mothers with children aged 6 to 23 months received a two-month supply of MNP sachets (60 sachets) to test acceptability and explore uptake. Community health workers/agents de santé communautaire (ASCs) and peer health educators/maman lumières (MLs) provided mothers with support, sensitisation and education on the adequate use of MNPs and nutrition messaging. Concern Worldwide Burundi was invited to join this programme to assist in the implementation, sensitisation and education on the adequate use of MNPs.
Concern conducted a post-distribution survey (exit interviews and focus groups) in Cibitoke Province three months after the December 2014 distribution. The December 2014 target was 28,666 children, of whom 28,007 were reached. The survey evaluated the effectiveness of communication and messaging during MNP distribution, focusing on the level of knowledge and use of the product, storage, and perceived secondary effects of use, to improve the sensitisation component for subsequent phases of the project. Specifically, it examined:
- Were mothers with children aged 6 to 23 months who received MNPs able to use them correctly at home?
- What determinants influenced the use of MNPs among mothers with children aged 6 to 23 months?
A sample of 114 mothers was interviewed for the quantitative evaluation. A sample of 30 mothers, divided into six focus groups, was interviewed for the qualitative evaluation.
Findings from the post-distribution survey
The survey identified a number of positive outcomes. Most mothers perceived that their children were healthier and more energetic (see Figure 1). Mothers reported fewer bouts of child diarrhoea during the intervention period. Mothers had a positive perception of the product; all mothers said they would give their children MNPs again if provided. No significant cultural barriers were identified. The survey substantiated high coverage recorded (97.7%), and all mothers reported receiving MNP sachets free of charge from medical personnel.
The survey also identified a number of key barriers, which are closely interlinked:
1. Poor community mobilisation by ASCs and MLs;
2. Poor follow-up with mothers and health workers;
3. Lack of clarity of the communication/education pamphlet;
4. Mislabelling on packaging; and
5. Unclear messaging with regard to the treatment target group.
The survey suggests that poor community mobilisation was closely linked to insufficient training of ASCs and MLs, who play a critical role in the dissemination of information and mirroring of best practices in their communities. They received only one day of training on the adequate use and importance of MNPs one week prior to Maternal-Child Health Week; this was insufficient to allow full understanding of the process and MNP utilisation (a new intervention to them). The short period between training and distribution did not allow the support agents to conduct visits to homes in their communities to sensitise mothers prior to distribution. In addition, there was no well-defined follow-up strategy to encourage mothers to use MNPs and to answer any questions that arose during the two months following distribution.
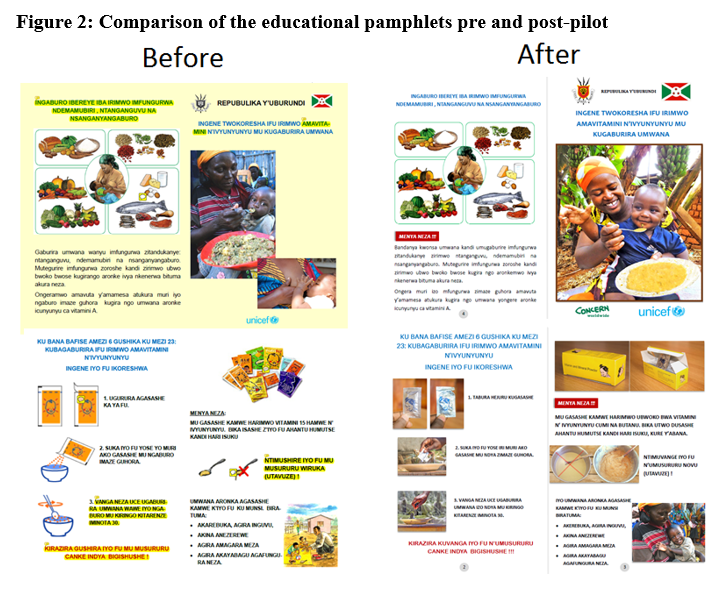
The education pamphlet contained two key messages on the use of MNPs and the importance of a balanced diet but failed to explain how these two are linked, and did not contain sufficient and clear information on the use of the sachets. For example, the survey revealed that mothers were not clear on the types of foods that could be used with MNPs. The pamphlet indicated that porridge was the food with which the MNPs could be used, leading mothers to believe that they could only be served over porridge. Additionally, the images used failed to communicate accurately the preparation process, resulting in confusion over the time between adding the content of the sachets to the food and feeding it the child, and the temperature the food needed to reach for the powders to be added.
The packages for the sachets displayed the incorrect age group, stipulating that the product should be consumed by children aged between 6 and 59 months rather than 6-23 months, resulting in mix-up among ASCs/MLs as well as mothers concerning who the product was intended for. The survey revealed that during the first day of distribution, MNPs were distributed to mothers with children aged 6-59 months, instead of those with children aged 6-23 months. Consequently, only 45% of mothers interviewed were aware that the MNPs should be given to children between the ages of 6 and 23 months, while 14.9% thought 6-59 months was the target age; 16.6% did not know; 15.8% were ‘other’; and 0.8% thought 0-6 months was the target group.
At the time of the post-distribution survey, three months after distribution, 64% of mothers still had leftover sachets; at the estimated rate of use (1/day), none should have been leftover following the two-month pilot period. The main reasons given by mothers for interrupted use were: they forgot (36%); the child was sick (24%); they were not present (18%); there was no porridge (15%); or they lost interest (7%). Mothers were uncertain whether MNPs could be consumed in tandem with medications and therefore stopped their use if their child became ill.
Recommendations and follow-up
Although there were problems around mobilisation, communication and labelling that affected uptake and use, distribution coverage was high and mothers had a high acceptance of the product, a good perception of its effects, and were willing to use it. Recommendations to address the identified barriers in future MNP distributions were:
- Better communicate general nutrition messaging and the role of MNPs in improving the nutrition status of infants (including improved health, reduction of diarrhoeal diseases and increase of child appetite);
- Incorporate clear messaging, outlining best practices for daily use of MNPs, in ASCs and MLs community mobilisation activities, and engage care groups and other community structures in such messaging;
- Correct the MNP packaging to reflect the target group (6 to 23 month-olds); and
- Improve the educational pamphlet to address mother’s questions and confusions and improve the quality of the images to better reflect correct preparation.
Concern subsequently worked with UNICEF to integrate these changes into the programme design and modify the pamphlet, using pictures rather than sketches to improve accessibility (see Figure 2). This was used in a cascade training by PRONIANUT, starting with national-level actors and reaching to community level, to enable the ASCs and MLs to sensitise mothers and teach them adequate use of MNPs more effectively. A new national packaging design will be used use for MNP supplies in 2016. Future rollout looks to integrate MNP distribution in the regular health system at both health facility and community levels. At the community level, the provision by community health workers will enable adequate coverage and good follow-up.
Conclusions
UNICEF and Concern worked together to identify weaknesses in the project and acted on them to improve subsequent phases of MNP distribution. This included investment by UNICEF and PRONIANUT in building the capacity of the ASCs and MLs. The experience highlights the importance of sensitisation, education and engagement of beneficiaries in planning and implementation; of stakeholder coordination and community involvement in building communication strategies; and of community awareness and sensitisation to relieve pressure on mothers. The project is a good example of how, through open lines of communication and feedback mechanisms, it is possible to overcome barriers, and how a project can be redesigned to have greater impact and improve the lives of the people it targets.
For more information, contact: Leni Martinez del Campo, email: lenimtz@gmail.com
1Burundi Country Profile. Global Nutrition Report 2014. http://globalnutritionreport.org/files/2014/11/gnr14_cp_burundi.pdf
2Nutrition at a Glance. World Bank. http://siteresources.worldbank.org/NUTRITION/Resources/281846-1271963823772/Burundi.pdf
3See previous footnote.
4UNICEF and the Micronutrient Initiative. 2004. Vitamin and Mineral Deficiency: A Global Progress Report and World Bank. 2009. World Development Indicators (Database), cited in http://siteresources.worldbank.org/NUTRITION/Resources/281846-1271963823772/Burundi.pdf