
Public health nutrition capacity: The quality of workforce for scaling up nutrition programmes
Summary of research*
Location: Global.
What we know: Priority for scaling up multi-sector programmes to tackle undernutrition in LMICs is growing. Public health nutrition (PHN) workforce capacity is critical to programme delivery.
What this article adds: A position paper by the World Public Health Nutrition Association (WPHNA) Capacity Building Task Force describes existing nutrition workforce capacity and potential mechanisms for building capacity (considering workforce size, organisation, and pre-service and in-service training) in LMICs. Nutrition-specific interventions are mostly delivered through health services that depend on decent staff ratios; community health workers are critical for impact. Guidance on multi-sector nutrition programming at scale is scarce, and estimates (where they exist) of PHN workforce numbers suggest they are inadequate. Applicable pre-service nutrition training is mostly clinical and/or food-science oriented; tools for in-service nutrition training largely relate to infant and young child nutrition and food security. Increased priority and funding for building capacity for scaling up nutrition is needed to realise global targets.
Introduction
Overnutrition and undernutrition problems affect at least half the global population, especially those in low and middle-income countries (LMICs). Programme guidance exists for undernutrition and overnutrition; priority for scaling up multi-sector programmes to tackle undernutrition in these contexts is growing. A position paper by members of the World Public Health Nutrition Association (WPHNA) Capacity Building Task Force outlines the case for and defenes the desirable characteristics of a system for developing the capacity of nutrition workforces for scaling up nutrition programmes in LMICs especially. It uses evidence from the literature and the joint experience of the Task Force to describe the existing nutrition workforce capacity and the potential mechanisms for building capacity. The World Health Assembly (WHA) has urged that member states should include a comprehensive approach to capacity building and workforce development in implementing plans for maternal, infant and young child nutrition, with the capacity indicator being the number of nutrition professionals per 100,000 population.
Key findings on the public health nutrition workforce
Nutrition programmes
Nutrition-specific interventions for reducing maternal and child undernutrition are mostly delivered through the health sector, while nutrition-sensitive interventions are delivered through other sectors such as education, agriculture, water and sanitation, and social welfare. Much less consensus has been created around interventions needed to reduce overnutrition. The importance of employing multi-sector approaches has been widely agreed, but documented experience of how such programmes are implemented is quite rare, with little or no guidance existing on how to develop and manage such programmes.
Many countries report having national, multi-sector nutrition plans, but very few of them are actually being implemented at any scale. Community-based health and nutrition programmes can be very successful, especially if they have the essential elements of community ownership, adequate population coverage, targeting, and central support for supplies and training.
To achieve impact requires a certain level of intensity of effort, with optimal ratios of not more than 20 mobilisers, or community health workers (CHWs) per facilitator/ supervisor and not more than 20 households per mobiliser. CHW volunteers typically receive some locally organised cascade training in order to be able to carry out their work, often from trainers who do not themselves have capacity to train health workers; there does not appear to be any national or international standard for these. Recent reviews confirm that CHWs provide a critical link between communities and health and social services and are effective at implementing evidence-based interventions.
Workforce structure
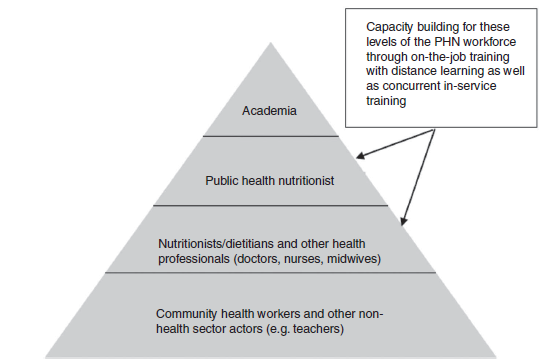
An ideal PHN structure includes a pyramid (see Figure 1), where the specialist PHN manager should have oversight of the delivery of all curative and preventive nutrition interventions delivered through the health system in the district. The delivery of such interventions is typically done by others, including nurses, midwives, dietitians and doctors. They in turn may provide support to other district actors, including CHWs, teachers, agricultural extension workers and social workers.
Figure 1: Multi-layered PHN workforce development1
Workforce size
Few estimates of PHN specialist numbers exist, but all suggest that they are either insuf?cient and/or largely missing in most national nutrition/health workforces. A recent survey of 13 countries in West Africa detected a critical shortage of skilled nutrition professionals in all countries, with limited supervision of nutrition activities, especially at implementation level by front-line health workers. Doctors, nurses and midwives (as well as dietitians in some countries) make up the majority of workers currently entrusted to deliver nutrition interventions globally, but training is particularly poor. For example, Asian regional country case studies (UNICEF and the WPHNA) concluded that the nutritional knowledge of health workers was outdated; their nutrition competencies were limited to more clinical and curative activities; and for nurses and midwives especially, their job descriptions did not include nutrition responsibilities. These findings are not surprising, since even in the USA and the UK the nutrition content of nurses’ and medical doctors’ training is also considered outdated and inadequate.
There is a lack of a dedicated workforce (especially in the health system) in most LMICs to provide outreach for community-based nutrition services. Scaling up CHWs was considered a crucial part of achieving the Millennium Development Goals (MDGs), but this did not happen.
Workforce organisation
Organisational diffculties are as great a hurdle to scaling up nutrition actions as the lack of PHN specialists, although the two are interrelated. No programme guidance exists that discusses dimensions of multi-sector nutrition programme governance; e.g. the need for a PHN specialist at all levels – in local government district planning office; in the central unit of each sector to oversee district-level implementation; and in the central unit to help plan, budget and oversee development.
None of the countries studied had in place a unifed nutrition information system that could guide decision-making processes for the double burden of malnutrition across the different sectors and levels of government.
A key challenge for scaling up community-based programmes is institutionalising and mainstreaming community participation. The largest and most successful programme is the Brazilian Family Health Programme, which has integrated 250,000 CHWs into its health services and institutionalised community health committees as part of municipal health services.
Workforce preparation
There does not seem to be any authoritative source of information (either regional or global) for graduate courses on nutrition. Programmes identifed in a survey of nutrition education in West Africa found that all of them failed to provide a comprehensive coverage of all essential aspects of human nutrition, being heavily oriented to food science (46%), with little emphasis on PHN (24%) or overnutrition (2%).
On-the-job training to develop the workforce to act in nutrition at scale will obviously require new and/or unconventional methods; e.g. a mix of distance learning and periodic coming together with tutors and mentors, which are both economically and logistically feasible.
Considerable material is available for in-service training of health-sector workers in the nutrition actions needed to improve maternal and child undernutrition; e.g. generic tools (such as counselling cards) for programming and capacity development of community-based infant and young child feeding (IYCF) counselling developed by UNICEF. FAO has also developed e-learning courses for professionals working in food and nutrition security, social and economic development, and sustainable management of natural resources.
Continuing professional development is another important area to be considered when developing the PHN workforce. Some universities offer online continuing education courses for nutrition and health-care professionals; e.g. the London School of Hygiene and Tropical Medicine’s distance learning course on multi-sector nutrition programming.
Improved availability of the internet has revolutionised the possibilities for capacity building in PHN. Initiatives include the Public Nutrition Virtual University (still awaiting funding) and the eNutrition Academy, a global nutrition-training platform (courses are still in development). Mentoring, defined as ‘a reciprocal, mutual and supportive learning relationship’, is one more tool that should be used to strengthen workforce development in PHN.
Conclusions
Unless increased priority and funding is given to building capacity for scaling up nutrition programmes in LMICs, maternal and child undernutrition rates are likely to remain high and nutrition-related non-communicable diseases are likely to escalate. A hybrid, distance-learning model for in-service training of PHN workforce managers is urgently needed in LMICs.
*Shrimpton, R., du Plessis, L.M., Delisle, H., Blaney, S., Atwood, S.J., Sanders, D., Margetts, B. and Hughes, R. (2016) Public health nutrition capacity: assuring the quality of workforce preparation for scaling up nutrition programmes, Public Health Nutrition, 19(11), pp. 2,090–2,100. doi: 10.1017/S136898001500378X.
1The pyramid structure represents numbers, not a hierarchical relationship.