
Multi-sector, nutrition-sensitive response to drought emergency in Pakistan
By Ali Dino Kunbher, Shafqat Ullah and Dr Mazhar Alam
 |
Click here to listen to an interview with the authors on the ENN podcast channel |
Ali Dino Kunbher is a Programme Manager for Welthungerhilfe (WHH) in Sindh, Pakistan, covering food and nutrition security. He previously worked with Action Against Hunger (ACF-International) and the Food and Agriculture Organization (FAO) and has an MSc in Agriculture.
Shafqat Ullah has been an Inclusion and Livelihood Specialist with Concern Worldwide since 2011. He has an MSc in Agriculture and over 17 years’ experience in agriculture, food security and nutrition-sensitive programming.
Dr Mazhar Alam has been a Health and Nutrition Advisor with Concern Worldwide Pakistan since 2015. He has more than 20 years’ experience of working with public sector, UN agencies and NGOs in the health and nutrition sectors and leads the national CMAM technical working group.
The authors would like to acknowledge the support of the funding donor, European Civil Protection and Humanitarian Aid Operations (ECHO).
Location: Pakistan
What we know: Undernutrition is multi-causal; nutrition-specific and nutrition-sensitive interventions are warranted.
What this article adds: A one-year, integrated, multi-sector project targeted communities at nutrition risk in an emergency response to drought in Sindh, Pakistan. Government departments at district level were engaged throughout. Nutrition-specific interventions involved community-based management of acute malnutrition (CMAM) and infant and young child feeding (IYCF) support. Nutrition-sensitive interventions involved seasonal cash for training, livestock assistance, improvement of communal wells and rain harvesting, and community hygiene outreach. The project aimed to target 80% of households with a malnourished child with nutrition-sensitive interventions in nutritional ‘hotspot’ villages. Positive impacts on access to CMAM treatment and IYCF support, livestock (milk production), hygiene practices and availability of safer water sources were reported. Beneficiaries increased expenditure on food and non-food items (especially agricultural inputs) and reduced use of costly, informal credit systems. Ambitious targets on water-borne disease and safe water access were not realised due to underestimated and challenging needs. Households successfully supported to build latrines (n=2,500) soon reverted to open defecation. Only one third of nutritionally vulnerable households were targeted by nutrition-sensitive interventions due to cost limitations. Informed by lessons learned, a follow-up project includes more livestock interventions, a community-led total sanitation (CLTS) approach and an exit strategy to sustain the CMAM programme led by government.
Introduction
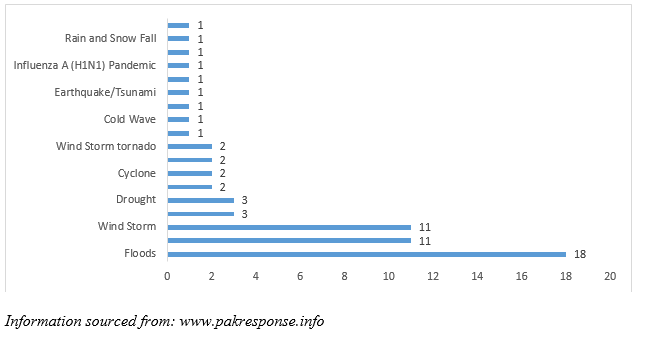
Pakistan, a lower middle-income country with the sixth largest population in the world, has an exceptionally high level of child undernutrition. According to the Global Nutrition Report 2016, stunting prevalence, at 45%, ranks 125 out of 132 countries, while wasting prevalence, at 11%, ranks 107 out of 130 countries (countries ranked lowest to highest); the country is sixth highest out of 185 countries in terms of anaemia prevalence (51.1%) (IFPRI, 2016). Pakistan is ranked 109 out of 118 countries on the Global Hunger Index (countries ranked lowest to highest score) (Global Hunger Index, 2016). One of the major contributing factors to the poor nutrition situation is natural disaster; a consequence of climate change, the country has experienced 63 natural disasters from 1935 to 2011 (Global Hunger Index, 2016) (see Figure 1). The frequency of drought affecting the country is increasing due to a gradual increase in temperatures. Thar Desert in Sindh Province has been most severely affected. It is an area covering 25,246 square kilometres with a population of 1,023,000 residing in two districts (Tharparkar and Umerkot). The area experienced a severe drought from 2013 until 2015 and recovery interventions are still underway.

In Thar Desert, 19.1% of children under five years old and 18.9% of pregnant and lactating women (PLW) are acutely malnourished (Concern Worldwide, 2016). Hundreds of children were reported to have died due to malnutrition over the last one and half years and 49% of large livestock and 59% of small livestock have died and/or been sold to try and meet immediate family needs (FSWGP, 2015). In terms of vulnerability, 68% of the population in the Thar Desert area fall under the category of poor and very poor (FSWGP et al, 2015).
Figure 1: Frequency of natural disasters in Pakistan from 1935 until 2011
Integrated multi-sector intervention
An integrated multi-sector project was developed to support nutrition at-risk communities in response to the continued drought emergency in Sindh, Pakistan. The project was designed by two Alliance20151 members; Concern Worldwide and Deutsche Welthungerhilfe (WHH), funded by European Civil Protection and Humanitarian Aid Operations (ECHO). The principal project goal was to improve resilience of the drought-affected population in Sindh Province. More specifically, the project aimed to meet immediate humanitarian needs of drought-affected communities through an integrated nutrition, food security and livelihoods (FSL) and water, sanitation and hygiene (WASH) response in Umerkot and Tharparkar Districts. Tehsil Umerkot in Umerkot District and Tehsil Chachro in Tharparkar District were selected as most severely affected by drought with high global acute malnutrition (GAM) prevalence. The project was implemented from May 2015 to August 2016.
- Provision of cash through cash for training (CfT) (nutrition, agriculture and livestock management) to the drought-affected malnourished households.
- Provision of livestock assistance, involving vaccination and deworming, livestock management sessions and clinics with the support of the government livestock department.
- Installation of solar-powered, water-pumping systems on existing communal wells.
- Construction of rain-harvesting water ponds.
- Hygiene promotion through community outreach workers.
Figure 2: Nutrition-sensitive geographic targeting process
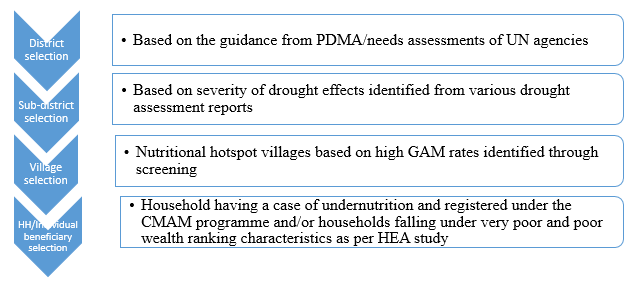
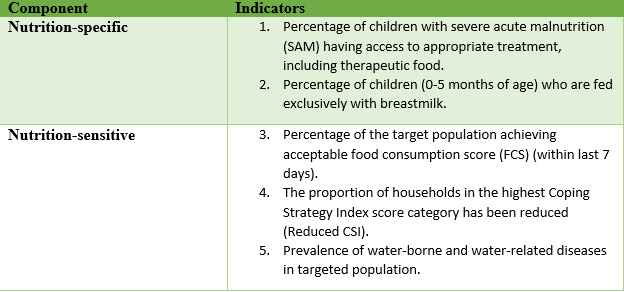
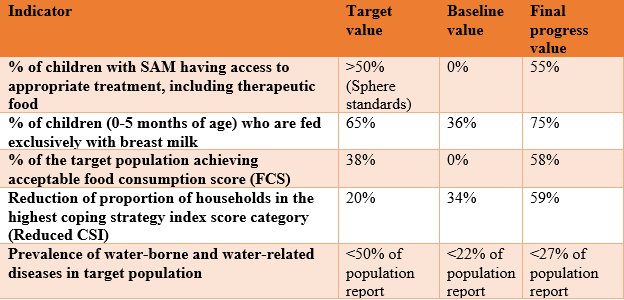
Table 1: Project indicators
Implementation process and impact of the project
CMAM/IYCF programme
Concern Worldwide implemented a nutrition-specific response, targeting children under five years old and PLW, involving CMAM service set-up, community mobilisation for uptake of health and nutrition services, and behaviour change communication (BCC) for improved IYCF and care practices. Quality treatment was provided to severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) cases and moderately malnourished PLW at the community level through mobile teams. SAM children with complications were treated in the stabilisation centres (SCs) established with the support of Concern Worldwide in the district headquarter hospitals. Orientation sessions (one-to-one and in groups) were held for mothers of malnourished children, caregivers, PLW and other women on topics such as breastfeeding, complementary feeding, ante- and post-natal care and personal hygiene. Breastfeeding corners were established at each CMAM static site for privacy and to provide mothers with counselling on IYCF-related issues. Mother support groups were also formed in each union council, comprising eight to ten women. These women were trained on screening of children and PLW and delivery of key messages on nutrition, FSL and WASH issues to women from their areas. During the project life, 61,693 children under five years of age and 27,494 PLW were screened. A total of 6,071 SAM cases, 11,395 MAM children and 9,201 malnourished PLW were treated in the CMAM programme.
Food security and livelihoods (FSL) programme
Food security and livelihoods-related interventions were designed to increase access of the targeted beneficiaries to adequate and diversified food through appropriate activities. The main activities under the FSL component were cash-transfer programing and livestock assistance.
Cash for training (CfT)
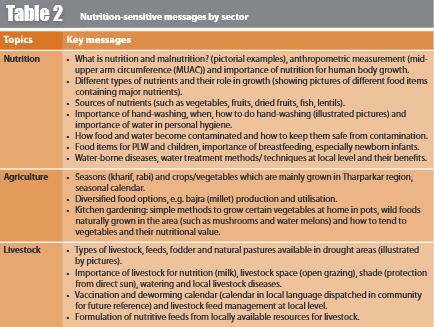
CfT targeted drought-affected malnourished households (referred from the nutrition programme), PLW and the most vulnerable people (those with disabilities and older people). It was designed to cover the extreme lean periods (September to November and March to August) when daytime temperatures can reach 50 degrees Celsius. The cash assistance was conditional on attending awareness sessions that delivered nutrition-sensitive key messages on nutrition, livestock and agriculture management; these focused on critical behaviours identified through a baseline knowledge, attitude and practices (KAP) survey (see Table 2). Each selected beneficiary received two days training on nutrition-sensitive messages followed by cash disbursement of PKR 6,000 (54 euros) per cycle through electronic mobile payment (Jazz Cash). There were three cycles so each beneficiary received a total of PKR 18,000 (162 euros). The cash amount was calculated based on the World Food Programme (WFP) food basket value for Pakistan. Cash disbursement was conducted in clusters near to the beneficiaries’ household, given the poor roads and transport facilities. The training time and duration was flexible in consideration of the target groups.
Table 2: Nutrition-sensitive messages by sector
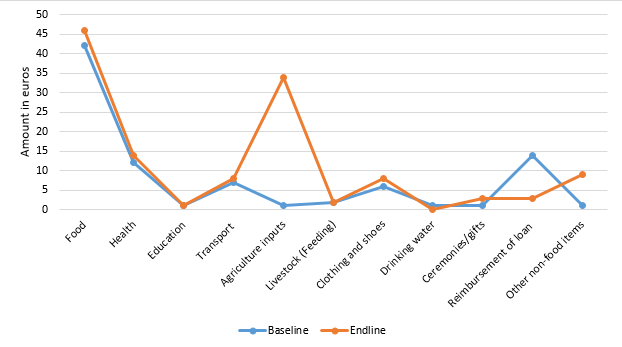
The baseline study found that, on average, beneficiaries were spending 88 euros on all monthly household expenses, including food, non-food and other expenses. At endline, monthly household expenditure was 128 euros, a rise of 40 euros, which is attributed to the cash assistance. Trend analysis shows that beneficiaries increased expenditures on food, health, agriculture inputs, clothing and other non-food items. The major area of increased expenditure was buying agricultural inputs for the forthcoming cropping season, while there was a considerable reduction in loans repayment; this suggests that those receiving cash switched to cash purchase in favour of the traditional structural credit system4 (see Figure 3). A total of 15,288 female individuals (PLW/child caregivers) were covered under this activity; males accounted for 6% (n=908) of beneficiaries.
Figure 3: Comparison of monthly expenditures (baseline and endline)
In Tharparkar and Umerkot most household livelihoods depend on rearing livestock (mainly small livestock). Heightened disease prevalence in drought conditions results in livestock mortality or weaker animals, for which there is a lower net return compared to healthy animals. To improve livestock immunity and good animal health, vaccination and deworming activities were planned with the support of the government livestock department for all targeted households in the area. Vaccination/deworming campaigns were organised at each village level where all small livestock (goats/sheep) and large livestock (cattle) were treated. The livestock of surrounding villages and communities were also covered to avoid any disease outbreak that may affect the project targeted areas. A total of 125,957 animals (102,468 small and 23,489 large) were reached through this activity. Beneficiaries reported positive impact on their livestock due to the vaccination/deworming assistance: 100% of beneficiaries mentioned increase in milk production.
Water, sanitation and hygiene (WASH)
Communal and household-level schemes were designed to improve community access to drinking water. In some villages, mostly females were responsible for collecting water from deep-dug wells (around 300ft) by pulling ropes in groups or using animals (donkey, camel). This laborious task and distance to the dug wells were creating health hazards for women, especially PLW, so solar-powered water-pumping machines were installed on a total of 12 dug wells. An additional 100 villages were identified from the hotspots for rehabilitation of depression sites5. Local villagers were engaged in the rehabilitation work through cash for work. The project also assisted 1,350 households from the same villages who had SAM cases, for construction of household underground water tanks. The tank is dual-purpose; for household water storage and to harvest rainwater during rains.
Hygiene promotion was integrated into all project-awareness sessions. Key messages included critical times and appropriate methods for hand-washing, personal and household hygiene and water treatment at household level. Hygiene-promotion campaigns, celebration of WASH-related days, hygiene-promotion activities in schools, and hygiene-promotion messages through trained community outreach workers were some of the main approaches adopted to improve behaviours. In total, 34,500 families were reached through the hygiene-promotion component.
The baseline study found that around 28% of the population had pit latrines in use. A total of 2,500 families were identified from the nutritional hotspot villages who did not have latrines and were defecating in the open. These families were supported for construction of low-cost latrines; latrine construction material was provided while they contributed voluntary labour. Despite this assistance and sensitisation on the importance of latrine use, use of latrines has not improved as much as anticipated. Although all 2,500 households constructed latrines and initially used them, many reverted to open defecation.
Coordination mechanism
Results/impact of the project
Table 3: Achievements of the project against set indicators
Lessons learned
Integrated, multi-sector, nutrition-sensitive programming to address the issues of malnutrition
Strong coordination among relevant stakeholders (UNICEF, WFP, Nutrition Cell, government line departments and local NGO partners)
Pooling different expertise of humanitarian sector brings drastic results
Synergies of the project with other interventions in the area
Imbalance between nutrition-specific and nutrition-sensitive interventions
Reduction in open defecation practices
Prevalence of water-borne and water-related diseases in targeted population
- Donor commitment to address recurrent drought and malnutrition.
- Local human resource pool (qualified local staff for project implementation were available in the area.
- Presence of relevant government line departments at grass-roots level, with active participation and interest of district administration in the project.
- Interest of provincial government in nutrition issues.
- Sensitivity to and involvement of the community; the project was designed to address immediate needs of the communities.
- Supportive social and cultural norms; Muslim and Hindu communities are equally represented in the area and welcomed the intervention, irrespective of diverse norms and religions.
- Streamlined procurement regulations to enable easier procurement by partners.
Conclusion
2IYCF activities were mainly nutrition specific, however, some IYCF messages were also covered by nutrition sensitive actions.
3An administrative division denoting a sub-district.
4A traditional conventional credit system prevails in the area, which communities use to get food and non-food items/or cash for household expenditure. It commands a high interest rate and whenever borrowers need a new loan (cash or in kind) they must adjust the existing loan.
5Natural places where rainwater gathers from the surrounding sand dunes. The land of that site is compressed and therefore its water-holding capacity is increased. Rainwater stands for long periods at such a site, locally called tarai (depression site.
6PHF is the coordination forum consisting of all the humanitarian international non-governmental organisations (INGOs) working in Pakistan.
7PDMA is a government body which takes the lead on all the disaster/humanitarian related work in the Province.
8The Cell is led by Department of Health, Government of Sindh and UNICEF.
9Cost per beneficiary was calculated by distributing the whole budget ‘programme + administrative’ per sector into the total number of beneficiaries covered.
References
International Food Policy Research Institute (IFPRI). 2016. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. Washington, DC.
Global Hunger Index 2016. http://ghi.ifpri.org/
Concern Worldwide (2016) SMART Survey Report, District Umerkot, January 2016.
Food Security Working Group Pakistan (FSWGP) (2015). Sindh drought needs assessment, 2015.
Food Security Working Group Pakistan (FSWGP), Concern Worldwide and Welthungerhilfe (2015) Household economy analysis.