
Realising rights and livelihoods opportunities among tribal populations in rural India
By Salome Yesudas
Salome Yesudas works as a consultant with several organisations on local food systems and nutrition-sensitive agriculture, specialising in uncultivated foods, millet-based food systems and agrobio-diverse farming systems.
The author would like to acknowledge Debjeet Sarangi, CEO of Living Farms, and Bichitra Biswal, programme officer for Living Farms, for their support in writing this article. The author would also like to acknowledge the support of Welthungerhilfe India. This article draws on content documented in a mid-term project progress report (Living Farms, 2014).
Location: India
What we know: Marginalised communities are particularly vulnerable to food insecurity and malnutrition.
What this article adds: Living Farms, a voluntary organisation in India, worked with 2,000 tribal households in 46 villages in Rayagada District, Odisha, between 2011 and 2017, targeting health, nutrition, agriculture, forest management and poverty alleviation. Baseline data reflected a poor community, with low literacy and education rates, poor access to government social protection schemes, poor uptake of antenatal care, excess infant and child mortality, and prevalent acute and chronic malnutrition. Working with government and harnessing traditional knowledge and practices, interventions included strengthening existing village institutions; development of kitchen gardens; promotion of dietary diversity and biodiversity through farming; and support for uncultivated food use. Mid-term review (2014) found improvements including greater access to government schemes and health services and improvements in dietary diversity and infant and young child feeding practices. Mortality rates and prevalence of acute malnutrition declined over the project period. Success factors include intersector collaboration between government departments and community mobilisation. Challenges included working within local power structures to negotiate changes in services.
Living Farms is a voluntary organisation founded in 2005 to improve food security and nutrition among marginalised farmers, landless agricultural labourers, forest-dependent communities and adivasis (indigenous, forest-dwelling communities) in Odisha, an eastern Indian state on the Bay of Bengal. Odisha is home to some of the poorest communities in the world; they are particularly vulnerable to food insecurity and malnutrition. Around 90% of communities that Living Farms work with in Odisha live below the national poverty line (Welthungerhilfe & Living Farms, 2011). This article describes the experiences of a Living Farms programme operating in Rayagada District, Odisha, over a six-year period (2011-2017). Rayagada District encompasses an area of natural beauty and covers an area of 7,073 km² (Figure 1). The population of the district is 831,000 (2011 census), is 86% rural, and comprises many races, cultures and languages. The district comprises 2,667 villages and is divided into 11 Community Development Blocks (CDBs) for administrative purposes. It has a literacy rate of 64% (72% male; 56% female) against a national average of 59.5%. The district is ranked 465 out of 599 districts in India (US-India Policy Institute, 2015).
Figure 1: Map of Rayagada District

Living Farms programme
The purpose of the Living Farms programme is to improve key indicators related to food security, income and nutrition status. It takes a holistic approach, addressing issues related to health, nutrition, agriculture, forest management and poverty alleviation. The Living Farms programme in Odisha is a six-year programme (2011-2017) that harnesses traditional wisdom and farming. Farmers grow and maintain their own seeds (using seed banks); use traditional ‘multi-cropping’ (rather than single cash crops) and natural/organic fertilisers; and market their own produce. Communities are supported through workshops, awareness programmes, technical farming support, village health days and food festivals to showcase community produce. The programme works closely with government officers from the Integrated Child Development Services (ICDS) scheme, health department officers, local government representatives and members of the School Management Committee (SMC). Living Farms started work with approximately 2,000 tribal households in 46 villages in the Bissamcuttack and Muniguda CDBs in 2011. This article describes some of the key intervention areas and progress captured in a mid-term (2014) project progress review (Living Farms, 2014).
Baseline study (2011)
A household survey on nutrition and education was undertaken in Rayagada District in August to September 2011; this served as a baseline for the Living Farms project. The survey was carried out by the Institute of Applied Statistics and Development Studies (IASDS), an India-based research institute, in partnership with Living Farms. IASDS provided technical support in data collection, analysis, reporting findings and making and applying recommendations. A total of 52 villages located in Bissamcuttack and Muniguda CDBs were covered and all households were targeted. Within households, target groups were pregnant mothers, mothers of children up to two years of age, children under five years of age (for nutritional status) and children aged five to 14 years (for educational status).
The study confirmed a predominately tribal population (92%), with the remaining minority made up of the Dalit1 people. The overall gender ratio among adults was 1,091 females:1,000 males and 943 females:1,000 males for children (no explanation is given for this gender discrepancy in the study report). The proportion of children under five years old was reported to be 8.5%, well below the expected under-five population of 14-15% based on the state birth rate. The infant mortality rate2 in the previous 12 months was 131 infant deaths per 1,000 (higher than the district infant mortality rate of 83 per 1,000). The major source of water in the area is tube well. Primary sources of income are wage labour (59.5%) and farming (39%), with people often involved in both. Migration for employment is low; only 293 migrations were reported in the last 12 months.
Access to government schemes was assessed, including ration cards, NREGA3 and school mid-day meals. Out of 2,010 households, 93% possessed a government ration card. However, availability of food from ration shops under the Public Distribution Scheme (PDS) was found to be poor, with 85% of households reporting having not received food from ration shops within the last month and 11.3% reporting having never received food from ration shops. NREGA was found to be almost non-functional; more than 58% of respondents could not get work even for one day and only 0.4% of 1,340 households who had participated in NREGA schemes were given a job for the recommended 100 days.
Education enrolment was found to be poor. Out of 1,873 school-age children, 65% were enrolled in school (of whom 54% were male and 46% were female). Major factors that discourage school attendance are family size, absence of teachers and poor quality of teaching. In a reported 69% of schools in the survey area, a mid-day meal was served, consisting of rice, dal, eggs and vegetables. Access to antenatal care, healthcare and services to treat acute malnutrition were not examined in the baseline study.
The nutritional status of women was assessed using anthropometric measurements, including Body Mass Index (BMI) and Mid Upper Arm Circumference (MUAC) (MUAC only was used for pregnant women). Of 138 pregnant women surveyed, 19 (13.8%) were malnourished, with MUAC < 21cm. Of 285 mothers with children under two years of age, 21% had a MUAC <21cm, of whom half (53%) had a BMI <18.5.
Nutritional status of children under five years old (693 children) was determined using height-for-age z-score (HAZ) as a measure of stunting, weight-for-age z-score (WAZ) as a measure of underweight, weight-for-height z-score (WHZ) as a measure of wasting and MUAC. While the prevalence of stunting was found to be extremely high (75% stunted, of whom 55% were severely stunted and 20% moderately stunted), cautious interpretation is necessary due to methodological flaws. Height was assessed using a tailoring tape in the baseline survey, with considerable possibility of data inaccuracy as a result. A height/length board was used in 2014 which should have improved accuracy but limits data comparability between studies (see 2014 mid-term study, reported later).
Nearly one quarter of children (23%) of children were wasted (12% severe; 11% moderate). About 62% of children were found to be underweight (34% severe; 28% moderate). Logistic regression analysis revealed that being in the age group 12 to 35 months and disease were major risk factors for malnutrition. Trend analysis based on single age revealed that underweight started accelerating from age eight months, peaking at 12 to13 months.
Programme activities
Strengthening of existing village institutions
The project has enabled 46 kutumb4 to access government schemes (such as the NREGA, old age pensions and strengthening PDS systems) and to ensure health and nutrition security among the community. Kutumb meet monthly for discussion among community representatives and to facilitate joint action pertaining to farming, health and nutrition. Village health and nutrition days (VHNDs) are organised monthly to promote access to health and nutrition services. On VHNDs, children who are identified as malnourished are referred to Nutrition Rehabilitation Centres (NRCs) to receive 15 days of treatment, coupled with feeding counselling targeted at mothers, and follow-up. Parents are given travel fares to attend.
Another important village institution supported by Living Farms are Women’s Rights Groups (WRGs), active in most of the project villages. WRGs consist of village women trained in the monitoring and identification of malnutrition and referral of severe acute malnutrition (SAM) cases, maternal and child health (MCH) programming (including prenatal, delivery and postnatal support, breastfeeding support, immunisations, nutrition awareness and education) and access to supplementary feeding schemes.

Progress assessed in 2014 found positive developments. MUAC was now assessed in 86% (19 out of 22) Anganwadi Centres (AWCs)5; this was previously not measured. Weight measurement and growth monitoring were being implemented in 15 VHNDs and weight measurement and haemoglobin count check-up of adolescent girls practiced in 18 AWCs. Service utilisation had also improved by 2014: 79% (161 out of 205) mothers accessed Janani Suraksha Yojana (JSY) 6 in 2014; 99% mothers had accessed MAMATA Yojana7 (60% in 2013 and 47% in 2012); 93% of pregnant mothers were receiving supplementary nutrition from Anganwadi centres; and 99% of children accessed complete immunisation during 2014. In terms of feeding and care practices, early initiation of breastfeeding was reported as practiced in 93% of infants; 78% mothers practiced handwashing before feeding their children; and 74% of infants under six months old were exclusively breastfed.
Promoting nutrition gardens
A total of 1,012 farmers out of 2,016 households from 46 villages were supported to develop nutrition gardens in their homesteads, growing 14 plant varieties, including fruits, greens, tubers and spices. Most farmers used their own seeds and did not use synthetic fertiliser or pesticide, instead using organic manures they prepared using local resources. Mid-term review found that, on average, each household harvested and consumed 40kg of green vegetables over a period of 45 days from September to October 2014. Nutrition gardens were also established during the project period in 12 village schools (out of a total of 28 schools in the target villages). SMCs and community members helped prepare the fencing and plough the land; children and teachers were also involved in the preparation process. Out of 12 schools, seven reported to have had a good harvest. On average, the schools harvested approximately 60kg of different varieties of vegetables, which were used in school mid-day meals over two months.
Promoting dietary diversity (DD) and biodiversity through farming
Living Farms promoted millet-based, mixed farming to replace cotton farming, with uptake among 1,350 farmers in the project villages on 1,850 acres of land with 35 to 40 crop varieties in each of the patches. These included 18 varieties of millet, nine pulses, four oil seeds and five tubers. Crop diversity was planned in line with the traditional food culture to enable a diverse, balanced diet that included carbohydrates, proteins, fat, vitamins and minerals.
Supporting the use of uncultivated food
Uncultivated food has been the major source of food for local communities for generations and conserving the traditional uncultivated food sources was central to the project. To this end, 38 of the project villages protested against commercial plantation of eucalyptus and teak, driven by the forest department, and advocated for the regeneration and conservation of the biodiversity of the forest. Twelve villages planted around 25,000 multipurpose trees in degraded parts of forest land, including mango, jack fruit, guava, black berry, mahua, barada saga, kendu and karanja. Around 65% of the saplings survived and are being cared for by the communities.
Village kutumb have sought to promote traditional foods to the younger generation through recipe festivals, where village elders share recipes, explaining the value of traditional foods for healthy living, and teach how and when to collect such foods. A national convention and exhibition on uncultivated food, ‘Food, Forest and Ecology’ was organised in New Delhi, where participants from across the country exhibited the rich heritage and diversity of uncultivated foods and demonstrated recipes. The Women and Child Development Minister and Secretary of the Ministry of Tribal Affairs attended the exhibition and a documentary film entitled I Can’t Give My Forest To You was released at the convention. This provided a platform for dialogue to consider the promotion of traditional ‘forest food’ as an important policy to tackle malnutrition.
The Government of Odisha, influenced by the Living Farms project, has incorporated the promotion of forest food/uncultivated foods into various state programmes in nine tribal districts as a strategy to address food and nutrition, with support from IFAD, WFP and DFID.
Promotion of dietary diversity
DD scores for all households in the project villages were documented in 2012, using FAO and FANTA standard dietary diversity assessment methods8(FAO & USAID, 2016). All available foods were listed and 16 food groups were formed by the community. DD scores for households were documented for three seasons (summer, rainy season and winter) and overall DD scores. Food groups were designated cultivated or uncultivated and according to nutritional value and colour. Foods were also broadly divided into ‘go foods’, ‘grow foods’ and ‘glow foods’. Based on these classifications, posters were designed incorporating information on micronutrient-rich foods, with specific food sources for calcium, phosphorus, iron, vitamin C, folic acid and beta-carotene, and seasonal food calendars.
The posters were printed in Oriya language and distributed to every household as a wall poster. Based on the same food list, pictures of the food groups were incorporated into an Indian flag that simplified the go, grow and glow foods message. These tools were also used as a basis for discussion in monthly kutumb and WRG meetings and promoted during VHNDs. The DD assessment was repeated in April 2017 and is currently undergoing analysis.
Mid-term survey (2014)
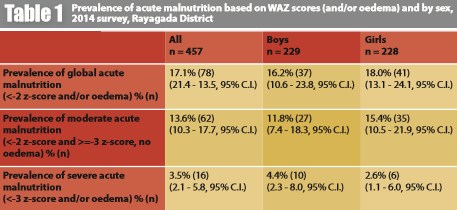
A mid-term survey was completed in August to September, 2014. Twenty-eight villages were surveyed, including anthropometric assessment of 457 children aged six months to five years. Overall sex ratio was 1:1; half the children surveyed (53.6%) were aged 6-29 months. Distribution by age and sex of the sample population is displayed in Table 1. The villages were selected from 52 baseline villages assessed in 2011, based on those villages with the greatest number of children under two years of age and pregnant and lactating women (PLW). The survey suggests a 13% reduction in the neonatal mortality rate9 (36 in 2014; 41 in 2011) and a fall in the infant mortality rate (131 in 2011 to 85 in 2014) over the three-year period. The prevalence of global acute malnutrition (GAM) was 17.1%; SAM was 3.5%, lower than the baseline in 2011 (23% and 11% respectively). The prevalence of moderate acute malnutrition (MAM) was higher in 2014 compared to 2011 (13.6% v 12%). Prevalence of stunting in 2014 was 57.4%. Comparative analysis between 2011 and 2014 is limited as there was no control group, and a different method to assess height was used between surveys that would impact on WAZ and HAZ indicators (see earlier). Confidence intervals are also not available for 2011 data to facilitate interpretation.
Discussion and conclusions
Under the Living Farms programme, 2,010 households from 46 villages were reached in the Ryagada District of Odisha, as well as 28 schools and 22 ICDS centres. Existing village institutions were strengthened to improve health and nutrition monitoring and access to government schemes. Dietary diversity was promoted among villagers and capacity-building activities were undertaken to improve farming techniques, establish nutrition gardens and promote biodiversity, conservation of forests and the use of uncultivated, traditional foods. A mid-term assessment indicated a decline in neonatal mortality and infant mortality over the initial programme period (2011 to 2014) and possible reductions in prevalence of GAM and SAM. While these data must be interpreted with caution, they suggest that the Living Farms programme has had a positive impact on the nutritional status of children in the area.
A key factor in the success of the programme is intersector collaboration. The programme brings together multiple government departments and facilitates meaningful collaboration around the goal of improved nutrition. As a result, several government programmes in the area became more ‘nutrition sensitive’. For example, the quality of the snack provided to children in the ICDS programme improved (they are now given a millet-based snack) and anthropometric measurements were more accurately taken due to improved oversight of the project. Also, education posters were provided to all ICDS centres and households, raising awareness of dietary diversity and nutrition. Living Farms has also built the capacity of government staff, such as Anganwadi community health workers, to improve service delivery within the population.
Community mobilisation is another important success factor. Using existing village structures, Living Farms has supported traditional systems, gaining community trust to plan and rapidly roll out programme activities within the population. Due to Living Farms activities, traditional farming practices and the use of uncultivated, forest foods were revived within the population; a key Living Farms success.
Key challenges of the programme were working within the local power structures; at times, these can hinder community action. Some traditional practices that had a negative impact on the health and nutrition of the community were deep-rooted and difficult to change. In addition, some government programmes ran contrary to the programme’s objectives and it was sometimes difficult to find agreement on the way ahead. For example, iron and folic acid tablets were distributed to mothers without proper dietary advice and education and without monitoring. Finally, there were important methodological flaws in both the baseline study in 2011 and repeat assessment in 2014 that limit the comparability of results and the extent to which changes can be attributed to the Living Farms programme. These should be addressed in future assessments to help understand the impact of the programme better.
In conclusion, a combination of local knowledge and up-to-date practices alongside effective communication tools and constant engagement of local communities have brought about positive changes in the diets of the local population to improve their health and nutrition.
For more information, contact Salome Yesudas salomeyesudas@hotmail.com
Endnotes
1 Dalit, meaning “oppressed” in Sanskrit, is the self-chosen name of this caste in India previously known as “untouchables”.
2 Deaths of infants under one year old per 1,000 live births.
3 Mahatma Gandhi National Rural Employment Guarantee Act, 2005. This offers to guarantee 100 days of wage employment per year to unskilled adult members of rural households.
4 Traditional village institutions.
5 A type of rural mother and child care centre and part of the government ICDS programme.
6 A government safe motherhood intervention in rural areas to reduce maternal and neonatal mortality.
7 An Odisha state scheme of conditional cash transfers to pregnant and lactating mothers.
8 A repeat of the DD assessment was carried out in April 2017. Results are forthcoming.
9 Deaths of infants aged 0-28 days per 1,000 live births.
References
FAO & USAID, 2016. Minimum Dietary Diversity for Women: A Guide to Measurement. Food and Agriculture Organization of the United Nations and USAID’s Food and Nutrition Technical Assistance III Project (FANTA), FHI 360 Rome, 2016. www.fao.org/3/a-i5486e.pdf; www.fantaproject.org
Living Farms, 2014. Realisation of rights and livelihood opportunities in rural India: Project progress report, July to December 2014.
US-India Policy Institute, 2015. District Development and Diversity Index. Accessed October 28, 2015. www.usindiapolicy.org/updates/general-news/225- district-development-and-diversity-index-report.
Welthungerhilfe and Living Farms (2011) Household economy approach Rayagada District, 2011, Fact Sheet, Working version 3. Vlker Lennart Plan, University of Marburg.