
A growth reference for MUAC-for-age among school age children and adolescents and validation for mortality
Summary of research1
Location: Kenya, Uganda and Zimbabwe
What we know: An internationally accepted reference for mid-upper arm circumference (MUAC) does not exist for school-age children and adolescents
What this article adds: Growth curves for mid-upper-arm circumference (MUAC)-for-age z-score for children age 5-19 years were constructed and evaluated against data from Uganda and Zimbabwe (ARROW trial) and Kenya to determine their discriminatory performance for subsequent mortality. The new growth curves transitioned smoothly with WHO growth standards at age five years. MUAC-for-age z-scores of −2 to −3 and less than −3, compared with −2 or more, were associated with hazard ratios for death within one year of 3.63 and 11.1 respectively (ARROW participants); and 2.22 and 5.15 respectively (Kenya). The area under the receiver operating characteristic curves (AUC)s for MUAC-for-age and body mass index-for-age z-scores for discriminating subsequent mortality were 0.81 and 0.75 (ARROW) and 0.73 and 0.58 (Kenya). MUAC-for-age z-score is at least as effective as BMI-for-age z-score for assessing mortality risk associated with undernutrition among African children age 5-19 years.
Introduction
The World Health Organization (WHO) recommends using body mass index (BMI) to assess malnutrition in school-age children, adolescents and adults. In 2007 WHO published growth references for weight, height and BMI for 5-19 year-olds; contrary to younger children, where MUAC is widely and increasingly used, MUAC was not included (WHO, 2007). A MUAC reference for US children and adolescents has recently been published, but at age five years, z-score values from −3 to 3 are between 0.6 cm and 2.6 cm higher than those of the 2006 WHO growth standards. There is currently therefore no internationally accepted reference, nor any studies that relate either MUAC or BMI to subsequent major health outcomes in this age group. The objective of this study was to construct growth curves for MUAC-for-age z- score for 5-19 year-olds that accord with WHO growth standards and to evaluate their discriminatory performance for subsequent mortality through a longitudinal cohort study.
Methods
The Health Examination Survey (HES)/National Health and Nutrition Examination Survey (NHANES) US population datasets (age 5-25 years), used to construct the 2007 WHO growth reference for body mass index (BMI) in this age group, were obtained. The HES cycles II and III and NHANES cycle I included data from 7119 children aged 6-11 years, 6768 children aged 12-17 years, and 23,808 people aged 1-74 years, respectively. For the HES datasets, all observations were initially included. For NHANES cycle I, observations from young people aged 5-25 years were included. These datasets were merged, giving a total number of observations from 20,953 individuals, then stratified by sex (10,639 females). Generalised additive models for location, scale and shape (GAMLSS) were fitted and measurements outside four standard deviations excluded. To achieve a smooth transition with the WHO growth standards at age 60 months, the authors imputed normally distributed z- scores for 36,000 hypothetical individuals, randomly assigned by sex and age and uniformly distributed from 24-71 months, which were then merged with the cleaned HES/NHANES datasets. MUAC was modelled, stratified by sex, as a function of age by fitting GAMLSS models and testing different transformations, including Box-Cox-Power-Exponential, Box-Cox-t, and Box-Cox-Cole-Green models.
The discriminatory performance for subsequent mortality of the growth curves was evaluated, firstly using data from 685 HIV-infected children aged 5-17 years participating in the Antiretroviral Research for Watoto (ARROW) trial in Uganda and Zimbabwe between 2007 and 2008. MUAC, weight and height were measured at baseline and dates of death or loss to follow-up were recorded. Secondly, a dataset was used of 1,741 children aged 5-13 years discharged from a rural Kenyan hospital (3.8% HIV-infected) 2007-2012, where anthropometry was routinely undertaken and recorded at admission. Both cohorts were followed up for survival during one year. Using the 2007 WHO growth reference, MUAC-for-age z-scores were calculated from the new growth reference and BMI-for-age z-scores. Hazard ratios for death were estimated using Cox proportional hazard models for predefined categories of MUAC-for-age and BMI-for-age z-scores. The proportions of children identified as malnourished by these MUAC-for-age and BMI-for-age thresholds were compared using a McNemar test. Multivariable models included age and sex (as well as HIV status for the Kenyan dataset, but not for the ARROW trial, as all children were HIV infected) as a priori potential confounders. To evaluate the predictive value of continuous MUAC-for-age and BMI-for-age z-scores, the area under the receiver operating characteristic curves were estimated for death within one year and differences in area under the curve (AUC) were tested.
Results
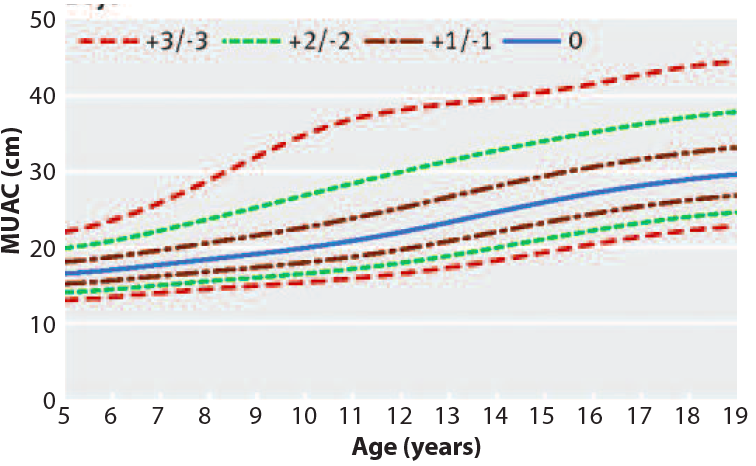
Figures 1 and 2 show the new MUAC-for-age z-score growth curves by sex. The new growth curves transitioned smoothly with WHO growth standards at age five years. MUAC-for-age z-scores of −2 to −3 and less than −3, compared with −2 or more, were associated with hazard ratios for death within one year of 3.63 (95% confidence interval 0.90 to 14.7; P=0.07) and 11.1 (3.40 to 36.0; P<0.001), respectively, among ARROW trial participants; and 2.22 (1.01 to 4.9; P=0.04) and 5.15 (2.49 to 10.7; P<0.001), respectively, among Kenyan children after discharge from hospital. The AUCs for MUAC-for-age and BMI-for-age z-scores for discriminating subsequent mortality were 0.81 (95% confidence interval 0.70 to 0.92) and 0.75 (0.63 to 0.86) in the ARROW trial (absolute difference 0.06, 95% confidence interval −0.032 to 0.16; P=0.2) and 0.73 (0.65 to 0.80) and 0.58 (0.49 to 0.67), respectively, in Kenya (absolute difference in AUC 0.15, 0.07 to 0.23; P=0.0002).
Figure 1: Mid upper arm circumference (MUAC)-for-age z score reference curves for girls aged 5 to 19 years
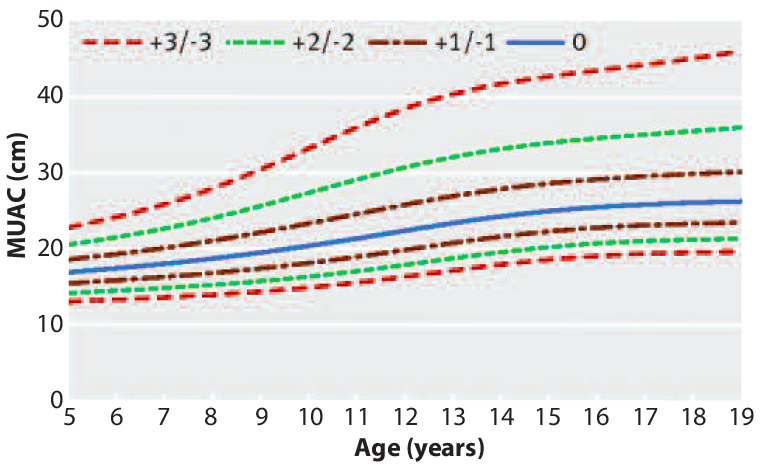
Figure 2: Mid upper arm circumference (MUAC)-for-age z score reference curves for boys aged 5 to 19 years
Results confirm that a new growth reference for MUAC-for-age among school-age children and adolescents can be used alongside WHO growth standards and is a valid anthropometric marker of the risk of mortality in HIV-infected and uninfected populations in Africa. The authors conclude that, with its practical simplicity and availability of reference curves, MUAC can be used in place of BMI to assess communities and guide treatment for individuals at nutrition and HIV programmes and as a standardised means of assessment in research.
Endnote
1Mramba L, Ngari M, Mwangome M et al. (2017). A growth reference for mid upper arm circumference for age among school age children and adolescents, and validation for mortality: growth curve construction and longitudinal cohort study. BMJ 2017;358:j3423 | doi: 10.1136/bmj.j3423
References
WHO (2007) Growth references for 5-19 years. Available from: www.who.int/growthref/en/