
Nutrition-sensitive agriculture in Zambia: A continued work in progress
Nutrition-sensitive agriculture in Zambia: A continued work in progress1
By Mary Corbett
Mary Corbett is a Nutrition Adviser for Self Help Africa (SHA), based in Dublin and supporting country programmes. Mary has around 25 years’ humanitarian experience working in health and nutrition with many organisations in various roles. She has a Master’s degree in Nutrition, a diploma in Tropical Medicine and a nursing background.
SHA is an international, non-governmental organisation working in ten countries in Africa, focused on supporting small-holder farmers to strengthen agriculture and enterprise. In the last five years a strong nutrition component has been embedded in newly funded programmes.
Location: Zambia
What we know: Integration of nutrition into agriculture programmes has mixed success in terms of impact on nutrition outcomes, such as stunting.
What this article adds: The Community Integration of Nutrition in Agricultural Programming approach was piloted by Self Help Africa (SHA) in Zambia between 2013 and 2017. It tested incorporation of nutrition into agriculture and enterprise programmes with smallholder farmers through a multi-sector approach, targeting 16,000 households focused on women, children and vulnerable groups. The approach involved nutrition-specific interventions (IYCF support, vitamin A supplementation), a strong WASH component (World Vision partnership) and agriculture (training to farmers on improving food security, diversity and storage). Programming was delivered through selected (wealth-ranked) and trained community groups. Impact was found on stunting prevalence in children under 18 months of age (reduction from 38.5% to 31.4% after two and a half years of intervention); the proportion of severe stunting fell; and there were significant improvements in antenatal care attendance, IYCF practices and WASH practices. Household dietary diversity also improved. Success factors include embedding nutrition within the community through basic nutrition and WASH training; converging agriculture and nutrition at household level; and close collaboration between the Ministry of Health, the Ministry of Agriculture and SHA. A strong agriculture programme and strong community buy-in from the outset laid the foundations for strengthening nutrition.
The author would like to acknowledge the hard work of the SHA team in Zambia, in particular SHA staff in Northern Province. Special recognition is given to Edward Meleki (Programme Coordinator) for all his support over the years. The author would also like to recognise and thank all other stakeholders involved in this programme, including the Ministry of Health and Ministry of Agriculture and Livestock (MAL). A special thanks to all the communities in Luwingu and Mbala districts. Finally, the author gives her sincere appreciation and thanks to Irish Aid for funding this innovative programme, giving the flexibility to SHA to adapt the programme to needs as they arose.
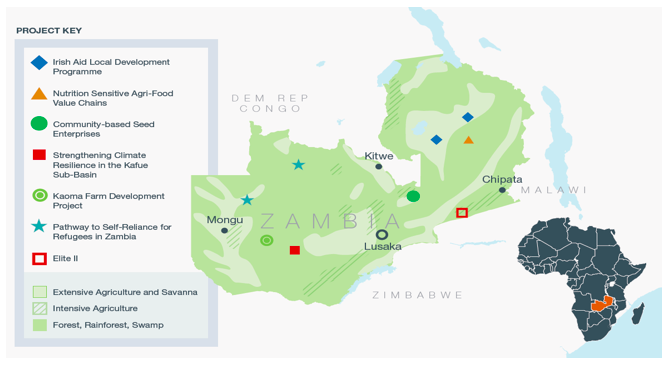
Figure 1: Map of key nutrition-sensitive agriculture projects in Zambia
Background
The CINAP (Community Integration of Nutrition in Agricultural Programming) approach was piloted by Self Help Africa (SHA), funded by Irish Aid, in Northern Province, Zambia (Irish Aid Local Development Programme) between 2013 and 2017 with a one-year extension in 2018 to support consolidation and exit. The purpose of the approach was to test the incorporation of nutrition into agriculture and enterprise programmes with smallholder farmers through a multi-sector approach. This was a development programme in two districts (Luwingu and Mbala), targeting 16,000 households (approximately 90,000 beneficiaries), with a focus on women, children and other vulnerable groups. The three objectives of the programme were to increase market-oriented sustainable agriculture production and productivity; improve the nutrition and health status of vulnerable households in the Northern Province; and improve service delivery to local communities by local authorities.
The CINAP approach
The current health centre-based focus of internationally driven initiatives to manage malnutrition largely focus on wasting reduction. Although integrating nutrition into agriculture programmes is not new, its success so far has been mixed in terms of impact on nutrition outcomes, such as stunting. Given this, the CINAP approach aims to place a stronger nutrition component within agriculture programmes at household/community level. For a multi-sector approach, the model also comprises a water, sanitation and hygiene (WASH) component to reduce the risk of illnesses, including gastric/diarrhoeal illnesses, which are known to further exacerbate malnutrition. Links are also developed with the nearest health centres for both curative and preventative healthcare.
Nutrition component
The core of this model is a combination of nutrition-sensitive and nutrition-specific interventions within agriculture programmes at community level, with a focus on women of reproductive age, infants and young children. Nutrition-specific interventions that can be undertaken at community level, which are key to the model promoted by SHA, include promotion of improved Infant and Young Child Feeding (IYCF) practices through the training of beneficiaries within the community and the formation of mother-to-mother support groups. Other interventions include support for vitamin A supplementation for children aged 6-59 months, supplied by health centre staff.
WASH component
An initial small WASH component included within the IYCF training was strengthened following the results of a knowledge, attitude and practice (KAP) survey, which showed poor personal, household and community hygiene and sanitation practices. SHA subsequently collaborated with World Vision (WV) and the Zambia Ministry of Water Sanitation and Environmental Protection to strengthen this component. WV initiated a community-led total sanitation (CLTS) approach, which complemented the community nutrition approach well. Emphasis is on aspects of improving environmental sanitation, construction of ‘tippy-taps’, improved latrines and drying racks, together with improved personal and household hygiene practices.
Agricultural component
Key components were integrated into the nutrition-sensitive agriculture intervention to support improved household food and nutrition security. Training was delivered to farmer groups using a training-of-trainers (TOT) approach, covering a variety of elements. These included production of higher quality and quantity of diverse crops with a specific focus on pulses and vegetables; improved small livestock husbandry; understanding of food groups and the need for a balanced diet; and better utilisation of food at the household level, in combination with developing local recipes and basic cooking demonstrations. Training on improved post-harvest handling and storage practices was also provided to improve shelf-life of food and reducing wastage and spoiling.
Programme implementation
Community groups
Following an initial contextual analysis and baseline study, a wealth-ranking exercise was conducted to assist with beneficiary identification. Within the identified communities, individuals were selected for participation in the programme (individual household methodology was used) and groups were formed, called Livelihood Enhancement Groups (LEGs). Each group comprised around 45 members, with an average of 60% female participants. Each group received initial training on group dynamics.
Different members within each group received specific training on a variety of agricultural/livelihood practices, including the principles of conservation farming, benefits of crop rotation, minimum tillage, education on intercropping and introducing new crops and better varieties. Members also received training on good practices in small animal husbandry. They were then tasked with cascading the training to others within their group. Some LEG members received inputs such as seeds and small animals (such as goats and chickens) to receive and pass on to others.
Evolution of nutrition component
The nutrition component of the programme evolved over time. Initially the programme collected data on dietary diversity (DD) using a modified World Food Programme (WFP) household Food Consumption Score (FCS) tool. The purpose of this was to gain an understanding of the variety of foods being consumed within households. The results from the FCS undertaken in November/December 2013 indicated that, in Luwingu, only 62% of surveyed households had an “acceptable” DD score (consuming a basic acceptable variety of food groups). Consequently, the first activities to be rolled out were promoting the production of a greater variety of foods and growing different varieties of pulses, small livestock rearing, and basic nutrition education.
In mid-2014 a KAP study was completed in Mbala district; a nutrition survey was conducted in Luwingu district in November/December of the same year. The results from these studies indicated that the nutritional situation was extremely poor, with levels of stunting in children under five years old at 53.4% and severe stunting at 26.6% in Luwingu district. IYCF practices were also very poor, with early initiation of breastfeeding at 53%, exclusive breastfeeding up to six months at 55%, and extremely poor levels of consumption of acceptable quality and quantity of complementary foods (17% and 48% respectively). WASH practices were also concerning. There was little understanding of the need to wash hands at critical times (before preparing food, before eating and after using the toilet) and how to make drinking water safe. There were also very high levels of illiteracy among women. Based on these results, it was decided that there was a need for a more comprehensive nutrition and WASH intervention within the programme.
The nutrition-specific IYCF training was considered a “grass-roots” training of community members (Figure 1). A six-day residential training was conducted. Initially one to two women from each LEG were trained, but over time it became apparent that a more gender-balanced approach was needed. Influential men were therefore included in the training at a later stage, with very positive results. This training was the official Ministry of Health (MoH)/UNICEF training usually conducted with health staff rather than communities, slightly modified by UNICEF/MoH and translated into local dialects (Bemba and Mambwe) by SHA (see Box 1). The training was conducted with groups of 20 by the official MoH/UNICEF master trainers. Informal feedback from staff, community members and MOH suggests the training empowers those trained, who are then recognised by their peers as having received significant useful knowledge. These IYCF-trained community members then conducted ‘cascade training’ with four to five other members each (mainly women) within their communities. This led to the formation of mother-to-mother support groups, through which nutrition information and training could be shared and cooking demonstrations provided to specific vulnerable groups.
Figure 2: Description of nutrition component of the programme

Box 1: Main components of the IYCF training
- Nutrition during pregnancy
- Early initiation of breast-feeding and importance of exclusive breast-feeding for six months, including the dangers of mixed feeding
- Good attachment to the breast and breastfeeding on demand
- Breastfeeding and working mothers
- Good hygiene practices
- Introducing complementary feeding – quality and quantity at different ages between 6 and 24 months (variety of foods, etc.)
- Feeding the sick infant and young child under six months and from 6 to 24 months and when to take them to a health centre
- HIV/AIDs and feeding infants and young children aged 0 to 24 months
- Growth monitoring
Over time, community IYCF-trained workers were linked with their nearest health centres and tasked with providing the centres with monthly activity reports. Some community IYCF trainers also attended the antenatal and under-five health days in their local health centre and provided support to health centre staff. Some community IYCF trainers also conducted nutrition screening at community level, doing regular mid-upper arm circumference (MUAC) screenings and referring children identified with malnutrition to the nearest health centre, or providing support and education to mothers and caregivers on nutrition within their community. Over 500 LEG members received the community IYCF TOT training; over 2,600 community members received cascaded training.
In addition to the strong general agriculture education within the LEGs, a component on growing vegetables and fruit trees (kitchen gardens) was added to the curriculum later, within the mother-to-mother support groups.
Results
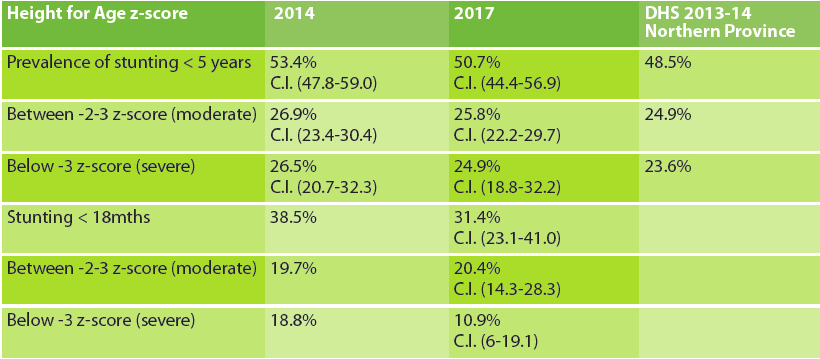
Several studies were completed to measure the impact of the various interventions in mid-2017, towards the end of the five-year programme. A repeat nutrition survey after two and a half years showed significant improvements in stunting trends among children under 18 months, with levels decreasing from 38.5% in November/December 2014 to 31.4% in April 2017 (Table 1). A change in the ratio of moderate to severe stunting was also observed. In the 2014 study the ratio of moderate to severe stunting was 1:1, while in 2017 this had changed to 2:1, meaning far fewer cases of severe stunting. Due to the overlap in confidence intervals it is not possible to say that the results are statistically significant. This may be due to two factors – the sample size of infants less than 18 months was small (119 in 2014 and 130 in 2017) and the timeframe was short between surveys (< 2.5 years).
A considerable change in stunting prevalence in children under five years old was not captured, but this is possibly also due to the short timeframe. In reality, the older children in the second study (over two and a half years) were likely to have been stunted before the CINAP intervention started and did not benefit from the stronger nutrition component.
Table 1: Self Help Africa nutrition survey results 2014 and 2017
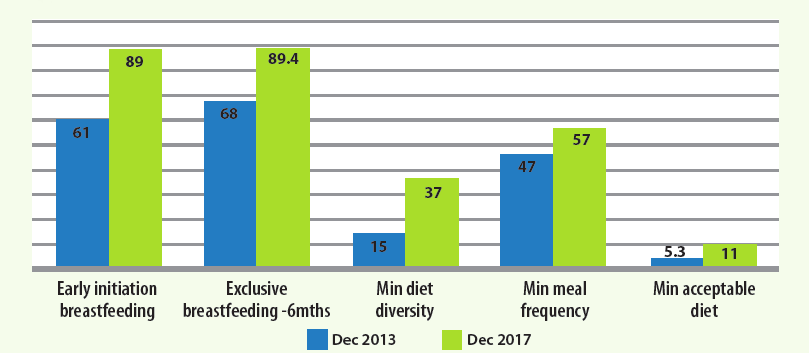
In terms of IYCF practices, some statistically significant improvements were reported in the repeat KAP survey, particularly in relation to pregnant women attending ante-natal services at least three times during pregnancy; mothers initiating breastfeeding within one hour of delivery; and exclusive breastfeeding to six months (Figure 2). There were also statistically significant improvements in complementary feeding practices, with increases in both the quantity and quality of meals provided to children aged from 6 to 24 months. Improvements were also recorded in WASH practices, including the use of latrines, ‘tippy-taps’ and drying racks. There was also a notable increase in the treatment of water to make it safe for drinking.
Figure 3: Self Help Africa KAP survey of ICYF practices in Mbala District
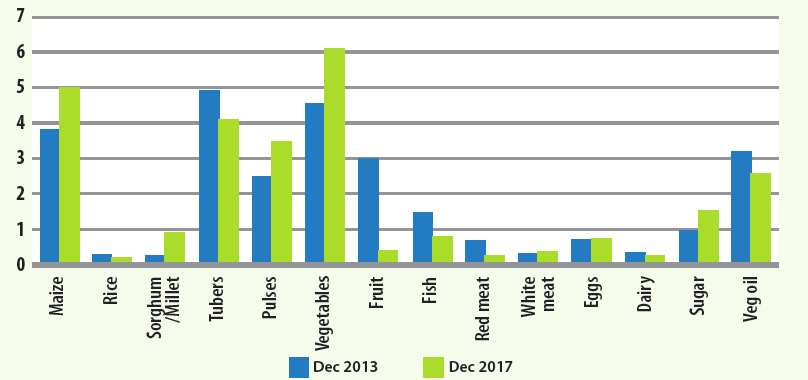
Household DD also improved over the lifetime of the programme. The introduction of pulses in Luwingu, together with training on their nutritional value and use, was an important factor. Between 2013 and 2017 the number of days pulses were being consumed within households increased from 2.2 to 4.6 days. This is particularly important as pulses are a nutritionally valuable crop, especially where the diet is lacking in other good sources of protein, such as fish, meat, eggs and dairy.
It is important to note that there are also seasonal variations in data, particularly where there is only one dominant harvest, and the population is dependent on what is available locally. These factors can affect FCS score results significantly. In 2013 the FCS was taken at the beginning of the hunger gap, while in 2017 it was taken towards the end of the hunger gap, when food was less available. This is particularly important where communities are hugely dependent on own produce for food needs and where markets are very limited, as is the case with Northern Province in Zambia.
Figure 4: Variety of Food Groups Consumed – April 2017 and December 2013
Lessons learned
Key lessons that have emerged from this initiative include:
- Embedding nutrition within the community through basic nutrition and WASH training – particularly IYCF practices – appears to have substantially improved nutrition and hygiene practices.
- Implementing both agriculture and nutrition interventions together helped connect these sectors, converging at the household level. SHA technical staff understood and supported both areas and the need for integration for maximum results.
- Integrating nutrition into agricultural interventions is fundamental to improving food security by improving quality, quantity and diversity of food and ultimately utilisation, contributing to improved nutrition outcomes.
- During this intervention, SHA linked with the MoH from the start in terms of training and resources/material adaptation. However, the programme was not linked at health centre level, which was a flaw in hindsight, although this was rectified as time went on.
- The programme was linked with the Scaling Up Nutrition (SUN) Movement in Mbala district as SUN was being established there. It took time for this relationship to evolve, partly because SHA was not a known health/nutrition stakeholder.
- A positive learning point was the use of a slightly modified version of the IYCF training material that was developed by the MoH/UNICEF, as well as their approved trainers. This led to the training being accepted and acknowledged by the MoH and ultimately added weight to the model and improved its sustainability. IYCF TOTs received certificates from the regional MoH.
- Training should be simple, basic and practical, particularly when targeting communities with poor literacy levels. Cooking demonstrations were highly appreciated.
- In future nutrition surveys the sample should possibly comprise children under 24 months old, rather than under 59 months old, as a substantial amount of malnutrition occurs within the first 24 months of life.
- Where a SUN initiative exists, linkages should be made to further enhance stakeholder coordination (SUN was being established in one district soon after the IALDP commenced; over time this helped to improve coordination).
Box 2 describes essential components of the CINAP programme to provide learning for other nutrition-sensitive agricultural programmes.
Consolidation and exit
The current final year is focused on consolidation and exiting from the community and health systems by the SHA nutritionist. Within the two districts there are 19 health centres (HC) and attached to each health facility is a Rural Advisory Committee (RAC). Initially, a mapping will be undertaken to get details on personnel in the HC and the RAC. Details will be obtained regarding whether the RAC is functioning and what support is required. Capacity-building will be done with the RACs where necessary on basic taking of minutes of meetings, giving some basic material. A two-day training/sanitation will be delivered with health staff and RAC members in each HC on the IYCF IALDP model. Training on use of height boards and MUAC tapes will be conducted and these materials supplied to each HC. Training on the nutrition community referral system will be conducted (screening and referring cases with low MUAC). The SHA nutritionist will also participate in the quarterly district nutrition coordinating committee (DNCC).
Conclusions
Several factors influenced the success of the programme in Northern Zambia. These include: the willingness of the local authorities to work with SHA and this development programme, which led to close collaboration between the MoH and the Ministry of Agriculture; the presence of SHA technical staff on the ground to support the programme; and the fact that a strong agriculture component aimed at improving food security was being implemented even prior to commencing the nutrition components2. A recent study conducted by SHA with staff and other implementing partners highlighted the importance of a strong agriculture element to support improvements in nutrition (improving food security strongly linked with improving nutrition). The community involved in the programme felt that by improving food security, it was possible to make improvements in nutrition practices. This laid the foundations for strengthening nutrition. Close collaboration with another NGO specialising in WASH was also key to strengthening those aspects in the programme through CLTS; again this component had a bottom-up approach – embedding it within the community.
Box 2: Essential components of the CINAP model of a nutrition-sensitive agriculture programme
- Context analysis: Starting with an in-depth contextual and stakeholder analysis to ensure that interventions are appropriate and respond to local needs and that relevant stakeholders are involved and well coordinated at the early stages of programme design.
- Nutrition-specific training: This training should focus on the nutrition and health needs of vulnerable groups within the community, especially PLW and children under 24 months old. Where possible, it should involve MoH/UNICEF-accredited trainers.
- Nutrition-sensitive programming: The integration of nutrition within agriculture programming is essential to improve food security. Increased production, diversity and utilisation of food, together with nutrition knowledge and behaviour change, are key to improving nutrition outcomes.
- Working with different line ministries: Working with government ministries across different sectors (especially the ministries of health, agriculture and local government) allows for a more comprehensive lens in approaching nutrition needs at different levels and increases the potential for real collaboration on the ground contributing to long-term sustainability and positive impact.
- Working closely with nutrition coordination committees at district and sub-district level: These committees should be established where they don’t already exist (often within the context of the SUN Movement) and should comprise members from the relevant line ministries at district-level, together with other stakeholders, including non-governmental organisations (NGOs). They should be tasked with planning and coordination of activities to support improved nutrition outcomes.
- Linking with community health centres: Community IYCF trainers should be strongly linked to their nearest health centre, as this collaboration ensures that health centre personnel are aware of community needs. In cases where the health centre capacity is limited, IYCF-trained people within the community are encouraged to support the centre, particularly during child health days.
- Simple monitoring and evaluation (M&E) tools: Simple M&E methodologies should be developed in collaboration with the MoH and should adequately reflect the activities being undertaken by IYCF trainers at community level. These tools should be submitted to the nearest health centre and shared with NGOs and other stakeholders.
- Gender inclusion: Ensuring equal participation of men and women in the programme is key. In particular, it is important to ensure that influential men within the community partake in the various nutrition training as this will support buy-in and lead to positive change; men need to understand that nutrition is not just a ‘woman’s issue’.
- Translating material into local dialect and use of pictorial/visual aids: Identifying diverse and creative ways to enhance knowledge transfer, including cooking demonstrations and role play, is important, particularly where literacy is an issue; having visual aids also gives further legitimacy to the community IYCF trainers.
- Promoting basic WASH practices: This should focus on the promotion of good hygiene and sanitation practices at individual, household and community level, including aspects such as hand-washing at critical times, safe drinking water, food safety (processing, storage), refuge disposal, and disposal of human excreta. Collaboration with stakeholders working on WASH systems and infrastructure should be pursued.
For more information, please contact Mary Corbett.
Endnotes
1This is a follow-on paper from an article published in FEX issue 51 (Feb 2016) titled Nutrition-Sensitive Agriculture in Zambia: work in progress.
2This was not intentional but proved to be a key element of success. Our recommendation would be for the two components to start at the same time.