
Ensuring pregnancy weight gain: An integrated community-based approach to tackle maternal nutrition in India
By Sreeparna Ghosh Mukherjee, Pia Sen and Dr Nagma Nigar Shah
Sreeparna Ghosh Mukherjee is Senior Programme Manager in the Health and Nutrition Unit of Child in Need Institute (CINI). She is a senior development professional with over 15 years’ experience in public health and nutrition, leading large-scale programmes with organisations such as CINI, GOAL and CARE.
Pia Sen is Monitoring, Evaluation and Documentation Officer for CINI. She previously worked as a project supervisor for Liver Foundation West Bengal and as a researcher for Pratichi Institute. Pia has extensive experience in evaluating and monitoring state-run programmes in health, education and child protection.
Dr Nagma Nigar Shah has a bachelor’s degree in dental surgery and a Master’s in Public Health. She currently works in the Health and Nutrition Unit at CINI, providing technical assistance across different issues in health and nutrition.
The authors acknowledge the support of the CINI in the implementation of this project, as well as HCL foundation (funding partner) and the Department of Health and Family Welfare and the Department of Women and Child Development of the Government of West Bengal.
Location: India
What we know: Maternal nutrition is a critical determinant of maternal health and the nutrition, health and wellbeing of children.
What this article adds: In 2018, Child in Need Institute implemented a pilot maternal nutrition project in 98 government integrated child development services centres in three districts of West Bengal, covering 182 pregnant women. Frontline health workers were trained to identify pregnancies as ‘nutritional risk’, including thin, severely thin, overweight, obese and anaemic. Routine food provision (daily cooked meal), iron-folic acid supplementation and nutrition counselling were strengthened. Participants were weighed monthly. Fifty per cent of participants were malnourished at registration (30.3% severely thin or thin; 19.7% overweight or obese). Average gestational weight gain (GWG) was 9.36 kg (against 10 kg target in line with national guidelines) and was highest in undernourished women. Prevalence of anaemia reduced by 12% by the end of pregnancy, with most improvement in normal body-mass-index women. Rate of low birth weight among infants born of the cohort was 16%; 90% of whom were from severely thin and overweight/obese mothers. Recommendations are to identify pregnancies at nutritional risk by 12 weeks for targeted nutritional support; monthly routine tracking of GWG; improved adherence to government pregnancy supplementation programmes; and improved guidance on community-based maternal nutrition interventions targeted to different risk categories.
Background
India has the highest number of malnourished children in the world. In 2015, an estimated 37.9% of children under five years old in India were stunted and 20.8% wasted (India DHS, 2015). The health and nutrition of a mother is a major contributory factor to the nutrition of her child throughout the lifecycle (Black et al, 2008; Victora et al, 2008). An undernourished mother is more likely to give birth to a low birth weight (LBW) infant, which increases that child’s risk of wasting, stunting and child mortality and, later in life, their risk of non-communicable diseases such as diabetes and high blood pressure. Stunting in childhood also leads to lower educational achievements and, for girls, increases the chances of them growing into women who will give birth to smaller infants themselves, perpetuating the intergenerational cycle of malnutrition (Victora et al, 2008). In one study, nutrition support provided to pregnant mothers and their children up to the age of three was associated with an 11% increased chance of that child acquiring a graduate degree, compared to children who received nutrition support between the ages of three and six (Nandi et al, 2008). Optimal maternal health and nutrition are also important for a woman’s own ability to lead a healthy life.
India’s maternal mortality rate remains high, at 130 per 100,000 live births. This must be halved within the next decade to reach the sustainable development goal. Furthermore, India has one of the highest prevalences of anaemia among pregnant women in the world, at 53.2%. Uptake of iron and folic acid (IFA) supplementation among women of childbearing age in India is low (28% in West Bengal; NFHS-4 2015-16), despite widespread distribution, due to apathy and common side-effects of nausea and vomiting. This is aggravated by a lack of dietary diversity in regular food consumption, tending towards high consumption of starchy foods (rice and potatoes in West Bengal).
Child in Need Institute (CINI)1 has been working in child, women and adolescent health and nutrition in India for 45 years. In 2017, CINI, with support from the HCL Foundation2, initiated a maternal and child nutrition project in three districts of West Bengal, focusing on the first 1,000 days (conception until two years of age). The aim of the project is to change community-level practices to tackle malnutrition by facilitating stronger links between existing government services and recipients in the community.

Pilot maternal nutrition intervention
As part of this project, a pilot maternal nutrition intervention was implemented between April 2018 and February 2019 to facilitate adequate pregnancy weight gain and anaemia control in three blocks in three districts of West Bengal: Nagrakata block from Jalpaiguri district; Suti-I block from Murshidabad district; and Falta block from South 24 Parganas district. The pilot intervention was implemented in 98 integrated child development services (ICDS) centres3 across these locations. ICDS centres cover a population of 500-700 and were selected rather than sub-health centres as the delivery platform as they are more accessible to the community. ICDS centres were selected in discussion with the block administration based on social group (higher concentration of scheduled caste/scheduled tribe/Muslim population); geographical accessibility (hard-to-reach areas); high prevalence of child malnutrition; and the presence of population pockets currently underserved by ICDS centres.
Selection of participants
All women in their first trimester of pregnancy during May 2018 from all 98 ICDS centres were included in the intervention, with no exclusions (n=210). Over time, there were instances of miscarriage, abortion and migration, reducing the final cohort to 182. The intervention involved the pregnant women and their families, plus 221 frontline health workers (FHWs), including all auxiliary nurses/midwifes (ANMs), accredited social health activists (ASHAs) and ICDS workers in the 98 ICDS centres and 47 sub-health centres covering them.
Intervention strategies
The intervention was implemented using an integrated community-based approach that emphasised home-based care and timely utilisation of government health and nutrition services by participants. Key strategies included:
Strategy 1: Identification and follow-up of pregnant women ‘at nutritional risk’
A pregnancy is considered ‘at nutritional risk’ if there are any nutritional deficiencies that can affect the pregnant woman’s health and the health of her child (both during pregnancy and the post-pregnancy period). According to the maternal nutrition services package in India,4 pregnancies are classified either as 1) not at nutrition risk (normal body mass index (BMI): 18.5-22.9, India classification); 2) at nutritional risk but no medical risk (as assessed by ANMs); or 3) at both nutritional and medical risk.
A pregnancy is also considered ‘at nutritional risk’ when at least one of the following indicators is present:5
- BMI (taken <20 weeks gestation) identifies woman as severely thin, thin, overweight or obese (Table 1);
- Age of pregnancy (below 20 and above 35 years);
- Body weight at the time of registration (40 kg or less);
- Height (less than 145 cm);
- Anaemia (severe anaemia: less than 7 g/dl, moderate anaemia: 7-10.9 g/dl);
- Inappropriate gestational weight gain (GWG) (<1 kg /month or >3 kg /month from second trimester onwards).
Under the current regime of pregnancy care in West Bengal, all indicators are measured routinely except for BMI, which makes it more difficult to identify and categorise pregnant women according to their nutritional risk and provide needs-based counselling. This intervention incorporated an initial nutrition and health assessment, including BMI assessment, to define nutritional risk more effectively. Nutrition assessment was initially carried out by the CINI team and later by trained ICDS workers and ANMs.
Table 1: BMI cut-offs (taken <20 weeks of pregnancy) to classify pregnant women at nutritional risk6

On identification of pregnancies at nutritional risk, a management plan was tailored to the specific needs of the pregnant woman. This included strengthened existing government interventions and new interventions, as follows:
Strengthened existing interventions:
- Increased home contact with pregnant women by the FLWs and CINI team to ensure timely uptake of antenatal check-ups and other services;
- Additional haemoglobin tests for anaemic women and follow-up for IFA supplement consumption;
- Ensuring ultrasonography examination of all women after second trimester (at the block hospital);
- Ensuring fourth antenatal check-up at the ninth month for all women by an ANM (at sub-health centres).
New interventions:
- Specific dietary counselling of pregnant women based on their nutritional status;
- Joint counselling of the family members of pregnant women to ensure support and sharing of household work burden;
- Monthly weight monitoring for assessing GWG.
Additional attention was given to severely thin and thin pregnant women who, together with their family, received additional home visits with repeated counselling on dietary diversity, quantity of food intake and the importance of rest. These women were followed up through home visits to encourage attendance at ICDS centres for daily food supplementation, monthly weighing and adherence to daily IFA supplementation. Those not gaining weight as per government guidelines (2 kg per month or over 3 kg per month from second trimester onwards)7 were sent for additional check-ups at the health centre to screen for complications. Ultrasonography was done for all cases in the second or third trimester to understand and detect abnormalities in foetal growth.
Strategy 2: ICDS-based interventions to ensure uptake of services
Certain innovations (not currently implemented in the existing system) were made at ICDS centres to support appropriate GWG, including:
Monthly weight monitoring:
The pregnant women were weighed monthly at the ICDS centre by an ICDS worker and counselled accordingly at that visit, with tailored messages to underweight and overweight/obese women. The routine practice in the state is to weigh pregnant women once per trimester at the health centre. GWG was calculated using the weight at the time of registration and the last weight taken before delivery. A target was set of 10 kg total weight gain during pregnancy, in line with government recommendations of 9-11 kg. International guidelines for GWG are higher, at 12-18 kg during pregnancy (IOM, 2009/WHO); however, studies demonstrate that women in India gain only about 7 kg on average for full-term pregnancy (Coffey, 2015) and reports from block-level officials, FLWs and communities suggest that average weight gain in West Bengal is lower, at around 5-6 kg. The decision was therefore made to lower the target, in line with government guidelines. While international guidelines recommend different levels of total GWG, depending on the pregnant woman’s starting BMI (underweight women 12.5-18 kg; overweight 7-11.5 kg; and obese 5-9 kg (IOM, 2009/WHO)), there is no such differentiation in Government of India guidelines and the setting of India-specific differentiated guidelines was felt to be beyond the scope and capacity of this study.
On-the-spot-feeding of supplementary nutrition and IFA supplementation:
In West Bengal, all pregnant women are provided with supplementary nutrition for six days per week from ICDS centres through provision of a hot cooked meal (usually a combination of rice, pulses, vegetables/soya-bean and one egg). This is usually taken home for consumption and shared within the household. To address this and low consumption of IFA tablets, spot-feeding of both supplementary nutrition and IFA tablets at the ICDS centre was implemented. Instead of taking cooked food home, the women were encouraged to stay at the centre to consume their meals, after which IFA tablets were also taken. This ensured that the women’s nutritional requirements were met and provided more frequent contact with service providers, and therefore greater opportunities for counselling. Women were initially reluctant to remain at the centre to consume the meal, partly due to lack of infrastructure at ICDS centres to support meal consumption. Repeated counselling helped change this practice in many of the sites.
Strategy 3: Working in an integrated, team-based approach
At the heart of this intervention was the convergence and collaboration of multiple community-level stakeholders to achieve the shared goal of improved pregnancy outcomes. A team was brought together at each centre of workers routinely responsible for the support of pregnant women and their families, including: ICDS workers, ASHAs, ANMs and self-help groups where present. Teams from each of the 98 ICDS centres were gathered for three different orientation workshops. Participative games were used to communicate the importance of team working, coordination and communication, and to unravel various myths and superstitions associated with pregnancy care. Simulation exercises created a sense of ownership and enthusiasm among the team in achieving the common goal together.
Incentives were provided to pregnant women to use all the services available to them in the form of coupons. On complying with each of the services in a timely manner, each pregnant woman received a coupon which also displayed a simple health-awareness message. At the end of the intervention, the pregnant woman and her family with the maximum number of coupons was recognised in front of the community as an example to follow. The best-performing team of FHWs was recognised in a similar way by congratulating team members at a ceremonial event organised by the block health administration. Feedback suggests that the coupons encouraged the families of the pregnant women to engage in the process and provide better support to them. Those provided to ANMs encouraged them to complete all ANC visits up the fourth scheduled visit on time.
Results
Initial assessment of the 182 pregnant women at registration during their first trimester revealed 50% to be malnourished. Of these, 30.3% were severely thin or thin and 19.7% were obese or overweight. Of the 182 women, 41% were married early (below 18 years of age at time of marriage); 16% were teenagers (below 20 years of age); 49% anaemic (haemoglobin levels below 11gm/dl at time of registration of pregnancy); and 70% were defined as having a ‘high-risk’ pregnancy.8
Gestational weight gain
The average GWG of the cohort was 9.36 kg, which is considerably higher than the average GWG of 7%. Sub-analyses by nutritional risk category showed that weight gain of 10 kg or more was higher in undernourished (severely thin and thin) pregnant women (Figure 1), and average weight gain was higher in this group compared to overweight and obese women (Figure 2). This suggests that counselling was appropriately tailored to the needs of the different groups according to their nutritional risk.
Figure 1: Percentage of pregnant women with GWG of 10 kg or more among different BMI categories
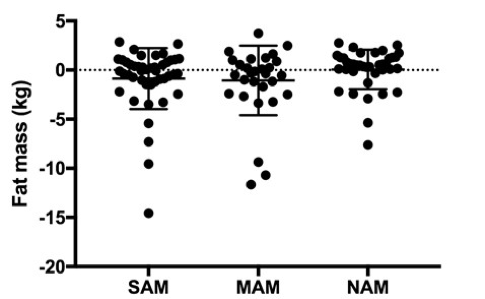
Figure 2: Average GWG among different BMI categories
Levels of anaemia
A 12% decrease in prevalence of anaemia in the cohort by the end of pregnancy was observed (Figure 3). Women with normal BMI were more likely to have improved haemoglobin levels (30%, compared to 14% and 22% of overweight/obese and thin/severely thin pregnant women respectively).
Figure 3: Prevalence of different levels of anaemia of pregnant women at registration and end of intervention
Birth outcomes
A high rate of deliveries (98%) took place in institutions (hospitals, nursing homes, etc), compared to the state average of 75.2% (NFHS 4, 2015-16). This can be attributed to intensive counselling and follow-up of the pregnant women and their families. The majority of infants born to intervention women (84%) had normal birth weights (2.5 kg or above); 16% (30 out of 182) of infants were LBW, compared to the prevalence of LBW in West Bengal of 11.5% (DLHS 4). Sub-analyses showed that prevalence of LBW was highest among severely thin and overweight/obese mothers, at 22% and 20% respectively, followed by thin and normal BMI at 15% and 18% respectively (Figure 4). A higher proportion of LBW babies were born to teenage mothers (30%) compared to adult mothers (26%). The prevalence of LBW among mothers with GWG of 10 kg or more was much lower (8%) than those with GWG of less than 10 kg (25%). This may point to the importance of GWG in improving birth outcomes.
Figure 4: Prevalence of LBW among different BMI categories
Another significant observation was that 90% of LBW infants were born to women with high-risk pregnancies. Among the different categories of high risk, 91% were anaemic, 77% did not gain weight up to 10 kg, and 62% had BMI that indicated malnutrition (undernourished or overweight/obese). This supports the literature that suggests that the prevalence of LBW increases in the case of high-risk pregnancies and low maternal nutrition.
Discussion
Results suggest that the intervention was successful in promoting weight gain among the women who needed it most (thin and severely thin pregnant women) and in reducing prevalence of anaemia among pregnant women. Results also emphasise the importance of focusing interventions on high-risk pregnancies in order to reduce the prevalence of LBW.
The intervention highlights the importance of proactively promoting appropriate weight gain in pregnancy among communities and health workers in India. GWG was rarely regarded as an important criterion for a healthy pregnancy and was not monitored regularly prior to the intervention. Key components that contributed to the success of the programme were collaboration between FLWs, promotion of GWG among FLWs and community members, and strategies to promote compliance among pregnant women to government supplementary nutrition and IFA programmes. Barriers such as distance to centres, lack of space to consume meals and resistance to IFA supplementation were ongoing challenges.
This programme also demonstrates the complex challenges that arise from implementing an intervention in the context of the ‘double burden of disease’, where malnutrition is present in all its forms within the same population (undernutrition and overnutrition, as well as micronutrient deficiencies). The ICDS programme as it exists now provides nutrition supplementation for all pregnant and lactating women with little scope for tailoring according to BMI, although nutrition counselling was successfully tailored to the needs of different nutritional groups in the intervention. National guidance on appropriate GWG according to maternal BMI is critical to inform future interventions.
Recommendations
Results of this pilot study call for actions that can be initiated concurrently at policy and implementation levels to promote optimal maternal nutrition:
Early identification of ‘at-nutritional-risk’ pregnancies at the time of pregnancy registration (by 12 weeks gestation) and subsequent follow-ups can help mitigate many risk factors in later pregnancy. BMI screening by ANMs is not routinely carried out in West Bengal for pregnant women and should be made mandatory in all sub-health centres.
Focusing on high-risk pregnancies would help to prevent LBW. However, currently no specific guidelines exist for managing high-risk pregnancies without medical complications at the community level. Guidance on a comprehensive package of community-level interventions to manage high-risk cases is needed.
Prioritising GWG. Monthly tracking of pregnancy weight gain should be integrated into routine systems. Appropriate counselling should be provided for GWG during different stages of pregnancy and for varied nutritional-risk classifications.
On-the-spot-feeding of supplementary nutrition and IFA. On-the-spot feeding at ICDS centres increases nutritional benefits for pregnant women and increases frequency of contact with FLWs and therefore counselling opportunities. This should be explored as an option for increasing adherence in other locations.
Development of a comprehensive package for community-based management of maternal nutrition. In addition to the above, a comprehensive package of interventions for community-level management of maternal malnutrition is needed that includes specific targeted guidance according to nutritional classification (including overnutrition and undernutrition). This will enable tailored programming and enhanced nutritional benefits for pregnant and lactating women in India.
For more information, please contact Sreeparna Ghosh Mukherjee.
References
Black R, et al. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet. 2008;371:243-60.
Coffey D. (2015). Prepregnancy body mass and weight gain during pregnancy in India and sub-Saharan Africa. Proceedings of the National Academy of Sciences of the United States of America, 112(11), 3302–3307. doi:10.1073/pnas.1416964112
District Level Household and Facility Survey (DLHS) 4 2011-2012.
Nandi A, et al. Early-life nutrition is associated positively with schooling and labor market outcomes and negatively with marriage rates at age 20–25 years: evidence from the Andhra Pradesh Children and Parents Study (APCAPS) in India. The Journal of Nutrition. 2018 Jan 1;148(1):140-6.
National Family Health Survey (NFHS-4) 2015-2016
Victoria CG, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340-57.
Endnotes
2 https://www.hclfoundation.org/
3 ICDS is a programme run by government in Indian states which provides supplementary nutrition, pre-school education, primary healthcare, and awareness of immunisation, health check-up and referral services for children under six years of age and pregnant and lactating mothers.
4 Maternal nutrition services package (Ministry of Health & Family Welfare (MoHFW), Government of India).
5 Ibid.
6 Ibid.
7 MoHFW maternal nutrition services package advocates for a weight gain of 9-11 kg during pregnancy, with no separate weight gain recommendation for overweight/obese women.
8 Indicators for high-risk pregnancy as per Government of India guidelines of ANM handbook. http://164.100.154.238/images/pdf/programmes/maternalhealth/guidelines/sba_handbook_for_anm_lhv_sn.pdf