
Zambia efforts in prevention, early detection and treatment of wasting during COVID-19
By Getinet Babu, Agnes Aongola, Colleen Emary, Phyllis Oyugi, Claire Beck, Chansa Tembo
Getinet Babu is a humanitarian nutritionist with over 16 years of extensive international and regional experience in emergency nutrition. He currently works as a Senior Humanitarian Nutrition Advisor with World Vision International.
Agnes Aongola is a Senior Nutrition Officer who has worked with the Ministry of Health for the past 28 years at various levels in nutrition, including responding to nutrition emergencies and participating in research activities.
Colleen Emary is a public health nutritionist with 19 years’ experience in international public health nutrition. She currently works as a health and nutrition Senior Technical Advisor with World Vision International, based in Canada.
Phyllis Oyugi is a public health nutrition professional with over 12 years’ experience working with international and national organisations in emergency and development settings. She currently works as a Nutrition Specialist with UNICEF in Zambia.
Claire Beck is a public health specialist with international nutrition, health promotion and health programme management experience. Claire currently works as Director of Humanitarian Health and Nutrition for World Vision International (WVI) and represents WVI in the Global Health Cluster and various working groups.
Chansa Nakazwe is the Nutrition Specialist for World Vision Zambia. She has over 10 years’ experience that includes working with the Ministry of Health and international non-governmental organisations.
The authors would like to thank the Ministry of Health for rendering full support to this project, including providing all the necessary data and project implementation, and UNICEF and World Vision Zambia for providing the necessary platform. The authors also acknowledge the health staff, programme staff and volunteers for making this project possible and contributing to the reduction of malnutrition in Zambia.
Location: Zambia
What we know: The COVID-19 pandemic and resulting movement restrictions have disrupted nutrition and health service provision in Zambia.
What this article adds: The emergency response plan designed to ensure adequate provision of nutrition services in response to a prolonged and severe drought in Zambia was at the conception stage when the COVID-19 pandemic began. Interventions were rapidly redesigned to include COVID-19 prevention measures and to ensure the continuation of service delivery at community-level and in nutrition centres. The government prioritised 36 districts where child wasting treatment services were initiated in 366 additional health facilities, totalling 647 of the 659 health facilities. Programme adaptations, such as the provision of personal protective equipment (PPE) and the adjustment of treatment guidelines or the strengthening of the supply chain, enabled the continuation of nutrition services for those in need and the resumption of outreach services. Between January and October 2020, a total of 6,361 children were admitted for treatment of wasting which reflects a 188% increase compared to the same period in 2019. As outreach activities resumed, the default rate in wasting treatment programmes dropped down to below 3% from 12% prior to the scale-up of nutrition services. Coverage during the child health week national campaign exceeded the targeted number of beneficiaries: over 3.5 million children under five years of age were reached, for a target of 2 million. These improved performances are thought to be due mainly to increased screening and the availability of services and the fact that the provision of PPE brought confidence to facility-based health workers and community-health workers to resume activities despite COVID-19 contamination risks. Preparatory steps are in place to initiate the screening for malnutrition by caregivers (Family MUAC approach) that will lead to the timely and early referral of children with acute malnutrition at outpatient therapeutic centres. The rapid integration of COVID-19 prevention activities into the nutrition programme, through the flexibility granted by donors to redesign project activities and the prompt implementation of these measures by partners, is regarded as a key success. A question remains as to whether or not this level of service provision will continue in the absence of further investment.
Background
Before the first cases of COVID-19 were confirmed on March 18, 2020, Zambia was already facing a serious food insecurity and nutrition crisis within a context of a fragile health system. Due to the devastating combination of prolonged and severe drought, the Zambia vulnerability assessment committee (ZVAC)/integrated phase classification (IPC) analysis published in August 2019 identified that 60 districts (out of the total of 116) had registered a huge decline in maize production, the main staple food in Zambia, and were projected to be in IPC phase 3 (n=57) and phase 4 (n=3) between October 2019 and March 2020 (IPC, 2019). In addition, the vulnerability assessment revealed an increase in severe acute malnutrition (SAM) levels in comparison to previous years in 24 out of the 87 districts assessed (OCHA, 2019).
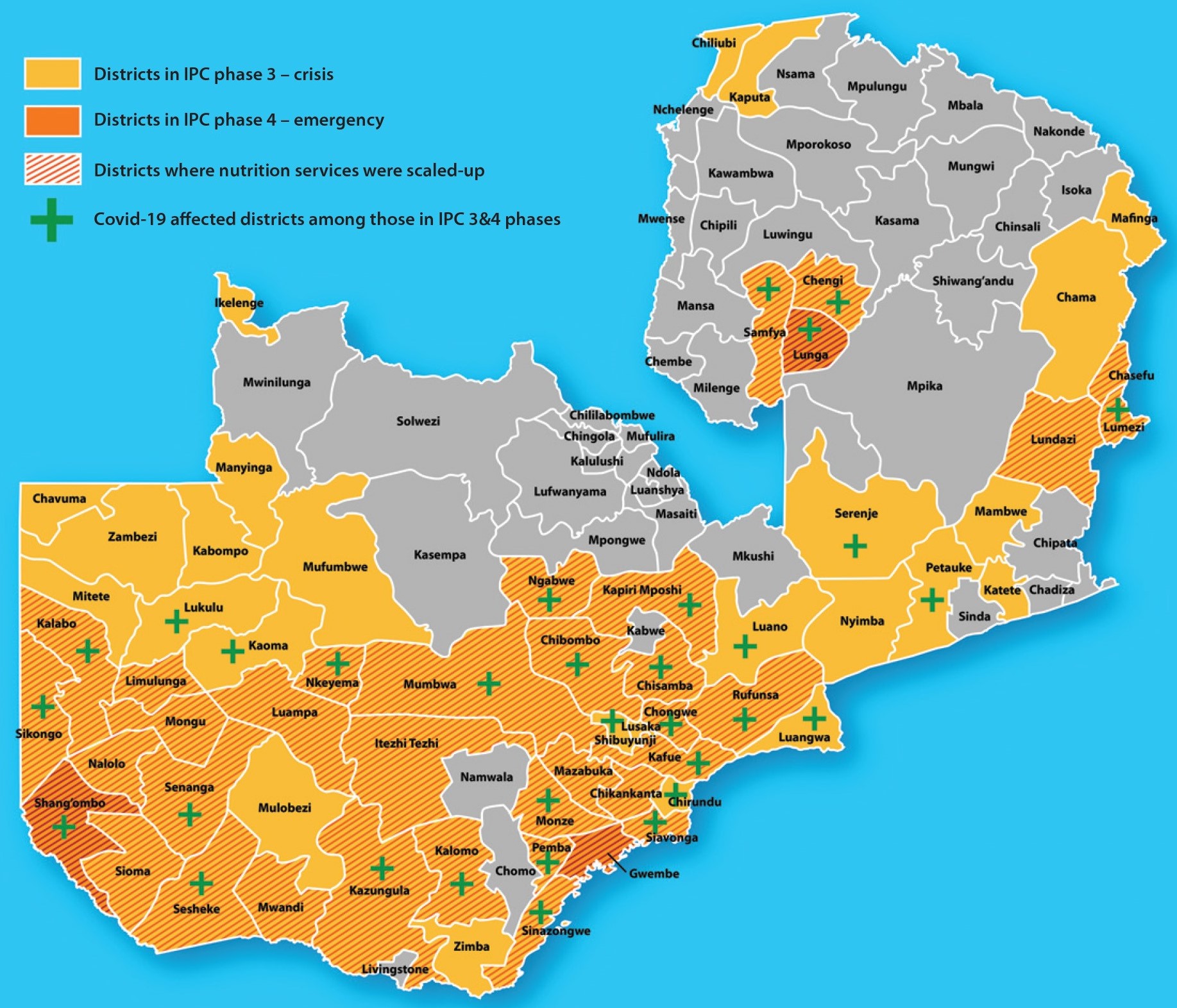
Of the 60 drought-affected districts classified as IPC 3 or 4, 36 were prioritised for the scale-up of malnutrition prevention and treatment services as of March 2020, driven by the Ministry of Health (MoH) and supported by UNICEF, World Vision, People in Need and PLAN International, with the remaining 24 districts continuing to receive routine integrated management of acute malnutrition (IMAM) services led by the MoH. When the COVID-19 pandemic began, this scale-up was in its conception stage. Interventions were therefore re-designed, adding additional scope, including the allocation of additional budget to include COVID-19 prevention measures at community-level and in nutrition centres. As of October 2020, 73 districts in Zambia were designated as COVID-19 affected (with confirmed positive COVID-19 cases) including 23 of the 36 districts prioritised for scale-up of nutrition services (Figure 1). This article describes efforts to support the continuation of essential nutrition services to prevent and treat child malnutrition and prevent the spread of COVID-19 in the context of the pandemic.
Figure 1: Districts in Zambia in IPC phase 3 and 4, districts prioritised for scale-up of nutrition services and/or districts affected by COVID-19
Scale-up and continuity of nutrition services during COVID-19
Coordination
The MoH led the coordination of the scale-up of nutrition services through the provision of key guidance and tools to health workers and the chairing of online nutrition partners meetings. This ensured that partners had a harmonised approach to the nutrition response and were updated on the latest guidance on nutrition in the context of COVID-19. All adaptations and scale-up actions detailed here were discussed and agreed upon in meetings and working sessions that included the MoH, UNICEF and implementing partners.
Scaling up nutrition services
In collaboration with the MoH and UNICEF, the three non-governmental organisation (NGO) partners (World Vision, People in Need and PLAN International) jointly developed a scale-up plan. Within the 36 target districts, wasting treatment services were initiated in 366 additional health facilities, adding to the 281 health facilities already providing services prior to the pandemic to cover 647 out of 659 health facilities. This ensured that wasting treatment service delivery was maintained despite the threat of COVID-19 and the resulting movement restrictions.
With UNICEF funding, the MoH and partners undertook a capacity mapping and a gap analysis in the 36 target districts (led by NGOs in 31 districts and by the MoH in five districts). These assessments identified that the capacity of health workers and volunteers was limited as a result of infrequent trainings and the absence of practical experience in implementing IMAM programmes. As a result, priority was given to improving the capacity of health workers and volunteers in IMAM and infant and young child feeding programmes as well as ensuring that appropriate infection prevention and control measures were put in place to make all stages of service delivery COVID-19 secure.
Timely reprogramming and financing
The allocation and availability of funds already designated for the 36 target districts, as well as additional funds from the Scaling-Up Nutrition (SUN) Movement Pooled Fund and the Foreign, Commonwealth and Development Office (FCDO),1 enabled the continuation and scale-up of essential nutrition services in the context of the global pandemic. This included a share of the USD200,000 allocated from the SUN II programme2 for the procurement of personal protective equipment (PPE) to support the COVID-19 response in the 73 districts that the MoH designated as COVID-19 affected. In addition, the UNICEF funds initially assigned to the emergency response in the 36 drought-affected districts were reprogrammed to include COVID-19 prevention activities within nutrition services. A greater focus was put on Lusaka district as this was the main hotspot for COVID-19, accounting for 60% of infection cases in the country. Both the flexibility and the additional allocation of funds for COVID-19 prevention activities allowed nutrition programming to continue.
Programme adaptations
To balance the demands of responding directly to COVID-19 and the maintenance of essential health service delivery, the MoH and partners designed a joint set of immediate actions which were initiated in April 2020. These included the following:
Introducing specific COVID-19 measures
Programme adaptations were introduced to wasting treatment services to comply with standard infection prevention control measures such as using PPE, strengthening hygiene practices and establishing community-based delivery platforms to handle movement restrictions. Community health workers (CHWs) and clinical staff received training in infection prevention control protocol measures by MoH, UNICEF and partners, including maintaining physical distancing, hand and respiratory hygiene and the cleaning and disinfection of equipment and the environment. The MoH, in coordination with UNICEF and other partners, including World Vision, provided PPE to all health facilities, including face masks, gloves, hand sensitiser, infrared thermometers and hand washing stations. Materials were also provided to CHWs for use during outreach activities, including boots and aprons. It was observed that the provision of PPE and supplies brought confidence to facility-based health workers and CHWs to continue to provide nutrition services in this new context. In addition, caregivers were instructed to bring their own cloths to use as weighing pants and mid-upper arm circumference (MUAC) tapes were disinfected between measurements.
Adjusting the IMAM guidelines
Rapid and temporary adjustments were made to wasting treatment protocols in the Zambia IMAM guidelines to enable necessary programme adaptations to continue treatment services. This included adaptations to the ration schedule for ready-to-use therapeutic food (RUTF) to cover longer periods whereby children with SAM without medical complications were given RUTF supplies to cover two weeks at a time, rather than one week. This helped to minimise overcrowding and reduced the frequency of caregivers’ visits to nutrition sites to reduce the risk of COVID-19 transmission.
Introducing the Family MUAC approach
To increase screening coverage, health workers and volunteers were trained how to take MUAC measurements for the detection of wasting and how to subsequently train caregivers to screen for wasting themselves (Family MUAC). The Family MUAC approach began being rolled out in December 2020 (later than anticipated due to initial shortages of MUAC tapes) and is anticipated to lead to the timely and early referral of children with acute malnutrition to wasting treatment services, at the same time as reducing the risk of COVID-19 transmission between volunteers and caregivers and their children.
Resuming outreach services
There was an initial drop in referrals of malnourished children to nutrition centres in the early stage of the pandemic, due to the temporary suspension of outreach services from March to June 2020 as well as caregivers fearing attending health facilities. These issues also led to suboptimal follow-up and increases in defaulting. When PPE became available, outreach services resumed and caregivers gained the confidence to attend health centres again. The district health office was also supported to develop plans to strengthen outreach and monitoring activities. This included provision of transport to facilities with remote outreach locations, provision of a stipend to volunteers who conducted community sensitisation activities and training, supervision and mentoring for CHWs. Through this programme, over 300 health workers and 721 CHWs were trained on programme adaptations.
As field monitoring was a challenge in the context of COVID-19, remote monitoring methods were adopted. The remote monitoring tools developed by UNICEF in response to the pandemic were tested and refined prior to rollout. In areas with good internet access, an online form was used. Where internet access was poor (five districts), information was collected through phone calls made by the district nutritionist to facility-based staff. A WhatsApp group provided a way to provide feedback and share reports for those who were experiencing network challenges. Key challenges of remote monitoring methods were delays in the submission of monitoring information and poor network coverage in some districts.
Ensuring a functional supply chain
The quick actions taken by MoH and partners to procure and donate PPE to each health facility gave health workers the confidence to continue the provision of basic health and nutrition services. In addition, efforts were taken to ensure sufficient RUTF supply with effective prepositioning of stocks in all districts. Health facilities were encouraged to monitor and timely report on their RUTF stock levels to help prevent stock-outs.
Ensuring continuity of the child health week campaign
Zambia, like many other countries, faced challenges in safely maintaining access to essential health services due to pressure on the health delivery system created by the COVID-19 pandemic. However, thanks to high community-level mobilisation and engagement, the child health week campaign (22-27 June 2020) was successfully implemented, ensuring the provision of major life-saving vaccinations and services. COVID-19 prevention measures in the context of child health week included use of a no-mouth touch approach for vitamin A supplementation, physical distancing with additional staffing for crowd control and the provision of handwashing supplies. Services provided during the child health week are presented in Figure 2.
Figure 2: Composition of the health and nutrition package of child health week
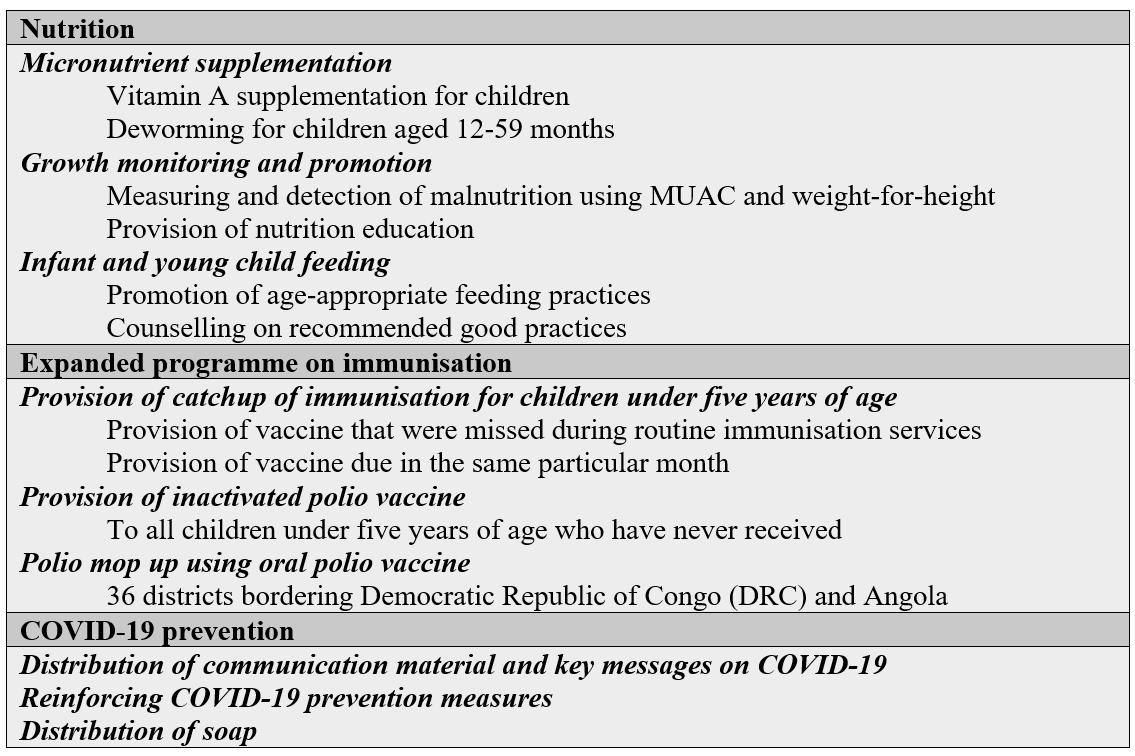
In addition to routine child health week activities – vitamin supplementation, deworming tablet, tetanus shots, provision of soap for handwashing – all caregivers and all mothers were reached with COVID-19 prevention awareness messages, along with lessons on safe motherhood and newborn care. The child health week campaign offered an opportunity to ensure that basic health services reached all targeted children especially those who do not benefit from routine health services.
Achievements
The rapid introduction of temporary adaptations to wasting treatment services was critical to ensure continued access to services in the context of the COVID-19 pandemic. It was observed that the provision of PPE and supplies brought confidence to facility-based health workers and CHWs to continue to provide nutrition services for those in need and enabled the rapid restarting of outreach services. Early transportation of RUTF to the health facilities helped to reduce RUTF stock-outs which enabled the continuation of wasting treatment services without interruption.
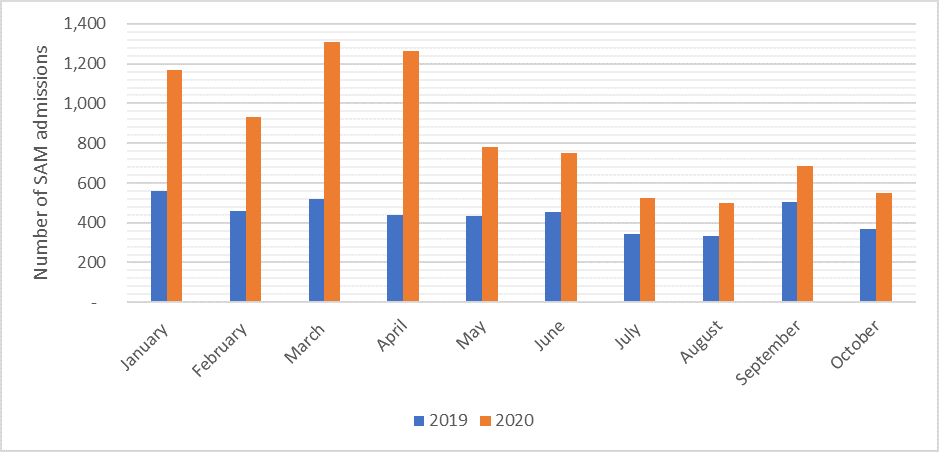
As a result of these adaptations, nutrition screening and treatment activities continued under COVID-19. Between January and October 2020, a total of 105,185 children were screened for wasting. Programme admission data in the 36 target districts indicate that a total of 6,361 children were admitted for treatment of wasting which reflects a 188% increase in admissions of wasted children compared to the same period in 2019 (Figure 3) (MoH, 2019 and MoH, 2020a). While it is expected that the drought conditions contributed to an increase in wasting cases, it is speculated that the increase in admissions is mainly due to increased screening and the availability of services, as outreach activities do not currently function well in routine IMAM services.
Figure 3: Number of monthly admissions for treatment of wasting before (2019) and during (2020) the COVID-19 pandemic
The defaulter rate for outpatient treatment of severe wasting treatment was 12% prior to the scale-up of nutrition services in the 36 prioritised districts, most likely a reflection of disrupted outreach activities due to COVID-19. In recent months, as outreach activities resumed, the default rate has dropped down to below 3%.
Maintaining the implementation of the child health week also demonstrated that it was possible to continue to deliver health and nutrition services while ensuring the safety of health workers and communities in the context of COVID-19. Despite occurring within the context of COVID-19, the coverage during this national campaign exceeded by far the targeted beneficiaries: over 3.5 million children under five years of age were reached, for a target of 2 million. This 178% coverage indicated a highly successful effort (MoH, 2020b).
Conclusions
The rapid integration of COVID-19 prevention activities into the nutrition programme, through the flexibility granted by donors to redesign project activities and the prompt implementation of these measures by partners, is a key success. A question remains as to whether or not this level of service provision will continue in the absence of further funding investments. The government’s investments in routine services exist but do not cover the full package of services, or do not cover all health facilities and outreach services. It is anticipated that treatment services will continue to be available in the facilities as part of the basic health service package; however, screening and outreach activities will probably not be sustained without additional funding.
Challenges also remain regarding supervision and data management. Innovative monitoring and reporting approaches need to be examined jointly by nutrition partners in order to increase health facility reporting despite poor internet network coverage in some areas of the country. In addition, it is important to better understand the implications of COVID-19 adaptations on routine indicators and wasting treatment outcomes, as the reduction in frequency of visits might negatively impact on the average length of stay and weight gain indicators. The definition of ‘defaulter’ also needs to be adapted to take into consideration the reduced frequency of visits. These are questions that need to be considered by the MoH and its partners when reviewing the routine programme monitoring data.
During the upcoming rainy season, the risk of flooding is expected to increase, affecting the north and north-eastern parts of the country, leading to disruptions to programme delivery. In preparation for these disruptions, more outreach sites should be added to continue the provision of services in the event that access to health facilities is cut off. Access to affordable, nutritious foods for maternal diets and adequate complementary feeding for young children remain severely threatened by the loss of income for the most vulnerable households. To address this challenge, government, development partners and the donor community should continue to invest in livelihood programming to prevent undernutrition while continuing wasting treatment services for all who need them. While these initial scale-up efforts have focused on the treatment of wasting, nutrition implementing partners and the MoH should strengthen the implementation of additional essential nutrition actions for the prevention of malnutrition including strengthening services for the promotion, protection and support of infant and young child feeding.
As this article is being finalised, COVID-19 cases are continuing to rise as are the number of districts reporting COVID-19 infections (from 68 in September 2020 to 96 in November out of 116 districts countrywide). Adding up the socio-economic impacts of COVID-19, the depreciation of the Zambian kwacha and the continued rise in acute food insecurity, serious concerns remain for the health and nutrition status of women and children in Zambia.
For more information, please contact Getinet Babu.
Subscribe freely to receive Field Exchange content to your mailbox or front door.
Endnotes
1 Formerly the UK Department for International Development (DFID)
2 The Scaling Up Nutrition (SUN) Programme is a cross-ministry and multi-donor programme to reduce stunting in Zambia. The National Food and Nutrition Commission (NFNC) implements SUN as part of the Government of the Republic of Zambia (GRZ) 1,000 Most Critical Days Programme. SUN 2.0, the second phase of the programme, has three major components: (1) Pooled Multi-Donor SUN Fund, (2) SUN Technical Assistance (SUN TA), and (3) SUN Learning and Evaluation. The Civil Society Alliance in Zambia, in collaboration with other SUN Networks, used SUN Movement Pooled Funds to lobby the government and to advocate for a system-wide approach to the pandemic that went beyond the health sector.
References
IPC. (2019). Zambia: integrated food security phase classification -Acute Food Insecurity May - September 2019 and Projection for October 2019 - March 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/IPC_Zambia_Acute%20Food%20-Insecurity_2019May2020March.pdf
MoH. 2019. Zambia MoH Ministry of health routine IMAM data 2019. and 2020
MoH. 2020a. Zambia Ministry of health routine IMAM data 2020.
MoH. 2020b. Zambia child health week preliminary data 2020.
OCHA. (2019). Zambia humanitarian response Appeal October 2019 - March 2020. United Nations Office for the Coordination of Humanitarian Affairs, published 24 Oct 2019. https://reliefweb.int/report/zambia/zambia-humanitarian-appeal-october-2019-march-2020
WHO. (2020). Maintaining essential health services: operational guidance for the COVID-19 context: interim guidance, 1 June 2020. World Health Organization. https://apps.who.int/iris/handle/10665/332240. License: CC BY-NC-SA 3.0 IGO
Zambia Vulnerability Assessment Committee Results. (2019). https://reliefweb.int/report/zambia/zambia-vulnerability-assessment-committee-results-2019