
Multi-sector nutrition programming: ‘Nutrition Smart Villages’ in Bangladesh and India
By Sweta Banerjee
Sweta Banerjee is the Nutrition Specialist for Welthungerhilfe’s India country programme. She provides support to the food and nutrition security projects in India, Bangladesh and Nepal. Sweta holds a Master’s degree in Dietetics and Public Health Nutrition and has worked in the public health nutrition sector for the last 25 years.
This project was conducted with funding from the German Federal Ministry for Economic Cooperation and Development. The author would like to thank the project staff and management of Welthungerhilfe India, Bangladesh and Nepal. The involvement of the following partners was also critical in achieving results: in India, Mahatma Gandhi Seva Ashram, Darshana Mahila Kalyan Samity, Vikash Sambad Sanstha, in Nepal, FORWARD Nepal and Aasaman Nepal and in Bangladesh, Anando and Friends in Village Development Bangladesh (FIVDB).
Location: India and Bangladesh
What we know: High rates of undernutrition exist among infants, young children and women of reproductive age in India and Bangladesh.
What this article adds: Nutrition Smart Villages – a multi-sector nutrition-sensitive approach to address the multiple causes of undernutrition by supporting communities to plan and implement activities and access government entitlements to improve agricultural, water, sanitation and hygiene (WASH), nutrition and care practices – was implemented in 200 target villages in India and Bangladesh over 24 months. The results of the baseline and endline surveys in 50% of the project villages showed marked improvement in women’s and children’s dietary diversity and improvement in WASH practices. However, few gains were made in the reduction of child wasting, particularly in India. This may be due to the heavy workload of women in India compared to Bangladesh, low dietary protein and also a long dry season during which dietary diversity could not be maintained. Key lessons learned are the need for a multi-sector approach to create an enabling environment for behaviour change, the need to integrate programming into existing institutions and government services and the need to strengthen government systems and find ways to overcome capacity gaps. The next phase of the project will focus on context-specific actions to sustain and improve the gains made for scale-up through the government.
Background
Undernutrition among women of reproductive age is a major public health problem in India and Bangladesh. In both countries, the prevalence of anaemia is high among pregnant women, at 40% and 41% in India and Bangladesh respectively (Development Initiatives, 2020). Undernutrition before and during pregnancy puts women and their offspring at risk of adverse health outcomes and transfers the risk of undernutrition to the next generation. Levels of childhood undernutrition are also extremely high; in India and Bangladesh respectively, only an estimated 16.4% and 26.6% of children aged 6-23 months achieve minimum dietary diversity, 38% and 30.8% of children are stunted and 21% and 8.4% of children are wasted (Development Initiatives, 2020).
Poor water, sanitation and hygiene (WASH) practices are a major risk factor for undernutrition and negative health outcomes in both countries. According to the latest National Family Health Survey, 51% of households in India have no improved sanitation facilities (94% among the poorest households) and less than 50% of the population have access to safely managed drinking water (IIPS & ICF, 2017). In Bangladesh, open defecation reduced from 17.68% in 2000 to 0.27% in 2016, however, by 2016 only 47% of households had access to basic sanitation facilities (WHO/UNICEF, 2017).
The loss of crop diversity in South Asia is considered a major environmental and health concern. Traditional seeds are being replaced by high yielding/hybrid varieties and farmers are increasingly using monocropping (growing a single crop year after year on the same land) for increased cash income. The impact of climate change has led to an increase in extreme weather events including floods, cyclones, drought and heat spells which compound the challenges experienced by smallholder farmers and lead to increased food and nutrition insecurity. It is predicted that the collective economy of South Asian countries could lose 1.8% of its annual Gross Domestic Product by 2050, rising to 8.8% by 2100 as a result of the impacts of climate change (Ahmed & Suphachalasai, 2014).
This article describes a multi-sector approach used in rural villages in Bangladesh and India by Welthungerhilfe (WHH) and partners that aims to address the multiple causes of undernutrition by improving agricultural, WASH, nutrition and care practices using a holistic, community-led approach. The Nutrition Smart Villages project was carried out for 24 months in target villages in India and Bangladesh from September 2018 to August 2020. The results of the baseline and endline surveys are presented along with lessons learned.
Programme description
WHH first started applying a multi-sector approach in 2011 in the context of a long-term, rights-based programme, the ‘Fight Hunger First Initiative’. This initiative was designed through a consultative process with 10 Indian partners with a vision to develop a long term, low-cost project that would engage multiple stakeholders and that could be scaled up through government systems. The project aimed to attract long term financing from donors in order to implement the concept and generate evidence of its impact. To date, 15 partners across three countries (Bangladesh, India and Nepal) have tested this multi-sector approach which has now evolved into the ‘Nutrition Smart Villages’ concept.
The Nutrition Smart Villages approach helps communities to understand nutrition in practical terms and plan their agriculture practices, natural resource management, entitlements and livelihoods according to the nutrition needs of the family, particularly focusing on the nutrition needs of children and women of reproductive age (15-49 years). The project also aims to demonstrate to local government how existing government schemes in India and Bangladesh can be converged at household level to target support to its members that are most vulnerable to undernutrition. The hypothesis is that if families understand their nutrition situation and needs, have control over their own resources and are empowered enough to create a demand for their entitlements, then their members will be able to achieve optimal nutrition. The increased demand for services is in turn expected to stimulate adequate service supply thereby creating an enabling environment for good nutrition.
In India and Bangladesh, the Nutrition Smart Villages project is currently implemented in 100 villages in two districts of Madhya Pradesh in central India (Chhatarpur and Sheopur) and 100 villages in three districts of Bangladesh (Netrokona, Sirajganj and the Chittagong Hill Tracts). Districts and villages were targeted based on social and geographical exclusion, landlessness and other social vulnerabilities. The government schemes of primary interest to the project are the Poshan Abhiyan in India and the National Plan of Action for Nutrition under the Bangladesh National Nutrition Commission in Bangladesh. Links are also made in both countries with government departments of livelihoods and rural development, food and supplies, agriculture, horticulture, fisheries, animal husbandry and WASH, all accessed through the local administration. Strong links are also made with village assemblies for village planning and budgeting.
WHH’s India and Bangladesh offices implement the programme of work through local non-governmental organisations (NGOs) with support from WHH in the form of capacity building on project and financial management, skills development around implementation activities and project monitoring and evaluation. The programme requires minimal infrastructure support and focuses on skills and capacity building. Interventions carried out by the NGOs are described as follows.
Village-level interventions
In each Nutrition Smart Village, five evidence-based interventions are implemented in partnership with community and grassroots service providers.
Linking agriculture and natural resource management towards nutrition security
Linking agriculture and natural resource management towards nutrition security (LANN+) meetings are held within the villages, through which community members learn about agricultural practices and natural resource management to support nutrition as well as diet, childcare and WASH practices. Local service providers along with volunteers from local committee/self-help groups (SHGs)1 use Participatory Learning for Action2 techniques to deliver the sessions over a period of 12 to 15 months.
Sustainable integrated farming systems
Sustainable integrated farming systems, including nutrition gardens, are important agroecology-based interventions that enable households to use all the available resources including uplands, degraded land and fallow land to produce food for their own consumption. Every family is encouraged to develop their own nutrition garden to produce seasonal vegetables, legumes, roots/tubers, spices and fruits. Gardens are integrated with crops, trees, fisheries, aquatic birds and livestock so that all the resources are optimally used to increase diet diversity. Hunger periods are reduced through the promotion of millets and the use of root intensification, farm bunds, multi-layer farming and mixed cropping among other sustainable agriculture techniques. Reduced dependence on markets for staples and pulses during lean periods enhances the capacity of families to buy fruits, vegetables and animal products to increase household dietary diversity. Food preservation and storage is included in farm planning as well. This farming system also supports the use and protection of natural resources in the local environment and the use of uncultivated foods.
Nutrition-sensitive micro planning
Elected village members are trained in nutrition-sensitive micro planning skills after which they work with villages to develop plans that focus on the needs of families with undernourished women and children. These members support households to develop their own resource plans to maximise food production, income and sanitation facilities using existing resources. They also work at village-level to develop village plans, mandated by government and linked to village development budgets, which are a compilation of the household plans submitted to the village assembly for approval.
Nutrition behaviour change campaigns
Campaigns are designed to support families, especially mothers with undernourished children, to adopt care practices that support good nutrition. The government service providers, along with volunteers and SHG members, are trained to measure height, weight and mid-upper arm circumference. Children aged 6-36 months are weighed and height/length is measured in each village to identify undernourished children. Caregivers of children identified as undernourished receive counselling on infant and young child feeding, hygiene and care practices. This initiative is further strengthened through promotional activities and low-cost interventions such as nutrition gardens, hand washing stations, water filters and waste management. Under this activity, 15-day positive deviance camps are facilitated for the mothers/caregivers of children identified as undernourished through which they receive demonstrations of care practices, the making of low-cost nutritious food recipes, nutrition gardening (including composition, preparation of bio-pesticide and seed preservation) and preservation of foods for lean periods.
Strengthening institutions
Existing village institutions, SHGs and local committees within the village are strengthened by project facilitators to understand government entitlements and how to access them. By informing, up-skilling and motivating these village-level institutions, government service providers are held accountable and villagers gain access to all the services that they are entitled to. Members of the village institutions are also engaged as volunteers for the LANN+ sessions, nutrition awareness, village micro planning and integrated farming to ensure project sustainability.
Meso- and macro-level interventions
Activities also take place at the meso- and macro-level through local NGOs supported by WHH. Partner NGOs develop knowledge management platforms to facilitate exchange between communities and policymakers. They also work to build the capacity of elected representatives at gram panchayat/ward/municipality levels on nutrition-sensitive village micro planning and understanding government schemes and budgets. Platforms are also created at state and national level to facilitate networking between partner organisations and to lobby government on policy development and citizen rights at national level for local-level support. To support these activities, WHH has developed manuals, training videos and information, education and communication materials to support the training of community and service providers in scaling up services to new villages.3
Results of baseline and endline surveys
After 24 months of implementation, the project aimed to achieve a 15% reduction in wasting (measured by weight-for-height z-score) for children aged 6-36 months, a 30% improvement in the number of women of reproductive age attaining minimum diet diversity for women, a 40% improvement in children aged 6-23 months in target households attaining a minimum adequate diet and a 60% improvement in target households improving WASH practices.
To measure success, a baseline survey was carried out prior to implementation, from April to May 2019, followed by an endline survey after 12 months, carried out in May to June 2020. For the baseline survey, a sample of 10% of households with children aged 6-36 months was selected. Due to budget limitations, the survey was restricted to 50% of the project villages and random sampling was used to identify the 110 villages. Clusters from each of these villages were selected using ENA software and households with children aged 6-36 months were selected randomly. A total of 1,186 households were surveyed across both countries (Table 1). The survey was repeated at endline to measure change in key indicators.
Table 1: Sample households survey
|
Country |
Number of project villages |
Total population from project villages |
Number of households |
Number of children 6- 36 months |
Number of villages in the sample |
Number of households surveyed |
|
Bangladesh |
100 (3 districts) |
110,000 |
21,529 |
5,622 |
60 |
559 |
|
India |
100 (2 districts) |
112,084 |
22,091 |
6,284 |
50 |
627 |
|
Total |
200 |
222,084 |
43,620 |
11,906 |
110 |
1,186 |
Findings
Figure 2 presents the baseline and endline findings for each of the indicators outlined as project targets.
Figure 2: Baseline (2019) versus endline (2020) findings of the Nutrition Smart Villages project in India and Bangladesh
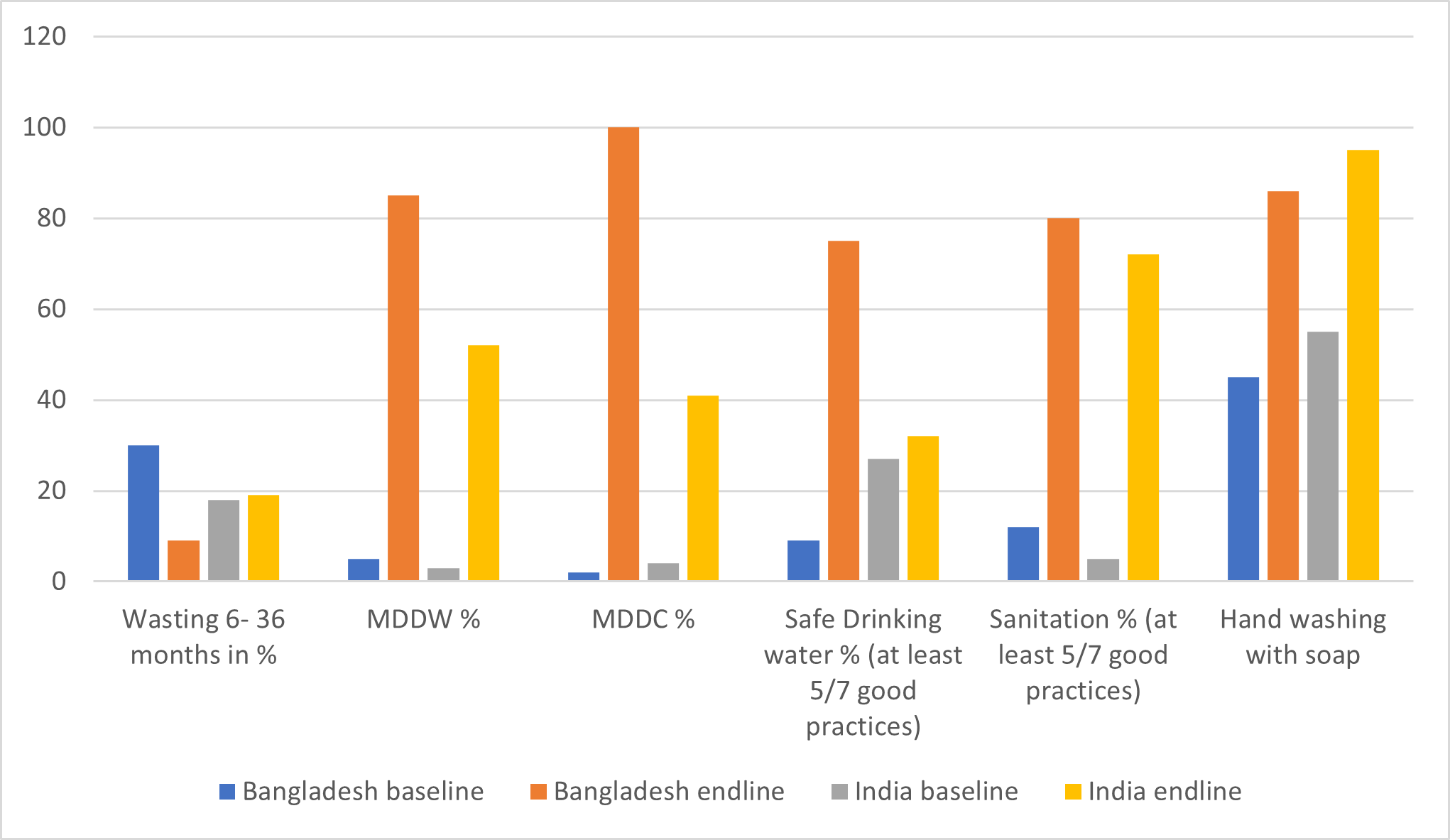
MDDW: minimum diet diversity for women
MDDC: minimum diet diversity for children
Child nutrition status
Results show that in Bangladesh the levels of child wasting in Nutrition Smart Villages were reduced during the project period, particularly severe wasting which reduced to zero. However, the number of cases in India did not improve and in fact rose slightly (Figure 3). Underweight data was also collected but has not been shared here given the short time frame between baseline and endline surveys; these results will be reported at the end of the next phase of the project.
Figure 3: Numbers and percentages of wasted children in target villages at baseline (2019) and endline (2020)
|
|
India |
Bangladesh |
||
|
|
Baseline |
Endline |
Baseline |
Endline |
|
Severe wasting (≤-3 WHZ) |
23 (3%) |
31 (4%) |
68 (12%) |
0 (0%) |
|
Moderate wasting (≤-2 and ≥-3 WHZ) |
99 (15%) |
150 (18%) |
82 (15%) |
80 (14%) |
|
Total |
122 (18%) |
181 (22%) |
150 (27%) |
80 (14%) |
Women’s diet diversity
The overall minimum diet diversity of women in the project villages improved dramatically in both countries. More than half of the target women were found to be consuming five or more food groups at endline compared to only 3% in India and 5% in Bangladesh at baseline. Although Bangladesh villages had a higher percentage of women consuming five or more food groups compared to India, both countries achieved over the target of 30% improvement in spite of the nutrition gardens being less successful in the Indian villages. Findings also show that own production as a source for cereals increased substantially; only 16% of respondents reported purchasing cereals from the market across all locations compared to almost 70% at the time of baseline. Respondents also reported increased consumption of animal products among those women farming animals including hens, goats and fish.
Children’s diet diversity
The proportion of children consuming four or more food groups increased from 4% at baseline to 41% at endline in India and 2% to 100% in Bangladesh. Children aged 9-23 months of age also showed 100% achievement in minimum meal frequency in Bangladesh but only a 9% increase from baseline in India in the same age group, and meal frequency in children aged 6-8 months actually decreased in India (15% at baseline compared to 7% at endline). The lack of increase in meal frequency in India may be as a result of strong social taboos and myths around complementary feeding. In addition, twice as many women from agrarian families are engaged in the agriculture sector in India than in Bangladesh, so the feeding of young children is often taken care of by older siblings or grandparents. Efforts are being made to popularise homemade instant mixes which are high in protein, carbohydrates and micronutrients to help to boost the nutrient intake of young children.
WASH behaviours
Access to safe drinking water has improved. In India, larger numbers of families now access private and public taps for drinking water (from 16% at baseline to 57% at endline). In Bangladesh, where the primary source of drinking water is handpumps, access to safe drinking water has increased from 42% to 89%. Hand washing knowledge and practices improved at household level from baseline to endline in both countries. Every household in Bangladesh has now installed an improvised tippy tap.4 In India, tippy taps have been installed at service delivery points but they are yet to take off at household level. Some households have been provided with hand washing stations but, due to scarcity of water knowledge, this has not translated into practice in terms of hand washing to the expected degree (nearly all respondents reported washing their hands after using the toilet but not at other key times such as after handling animals or before eating and preparing food). Positive change was seen in the use of toilets among households who already had toilets but were not previously using them.
Discussion
Over the course of one year, substantial gains were seen in project areas in both India and Bangladesh in terms of improved dietary diversity of women and children as well as in the adoption of improved WASH practices. There was some decline in levels of child wasting in project villages in Bangladesh but no improvement (and in fact a slight increase) in levels in India. The lack of expected change in child nutrition status may be as a result of the short implementation period (11 months). Poorer outcomes in India compared to Bangladesh may be driven by the fact that women in Central India are heavily engaged in agriculture, wage labour, migration and fetching water (more so than in Bangladesh) and therefore have less time for childcare which may compromise infant feeding practices. Variations in dietary practices between the two countries may be another cause; in India, the main protein sources are pulses and milk, compared to fish, eggs and chicken in Bangladesh. Project areas in Central India also have a very long dry spell during which water is scarce which affected the ability of many households to support dietary diversity throughout the year (in between the baseline and endline studies). A major limitation of these findings is that there was no control group; changes therefore cannot be definitely attributed to the project. That said, the impact on the quality of life of the project participants was readily observed by partners and has resulted in attention from governments and development agencies.
An important lesson learned from this programme is that increased knowledge can only translate into new behaviours in the context of an enabling environment including access to water, livelihood opportunities within the village, access to markets, improved infrastructure and the improved delivery of government services and good governance. To be successful, multi-sector programmes must be designed to integrate into existing community-level institutions and link to existing government schemes. This is what makes the programme scalable. The limitations of local government institutions in countries such as India and Bangladesh are a major impediment to sustainable change, in particular the lack of staff at grassroots level provides a major constraint to realising full government services. Strengthening local institutions and financially supporting volunteers were found in this context to be a suitable stopgap. Financial models are being explored to sustain this in the long term, such as service charges for volunteers paid by the community. The collection of data is also important to enable proper monitoring of progress. Data collection should focus not only on inputs and outputs but also results, for example, not just on whether toilets are constructed but the levels of open defecation, or not just on the development of nutrition gardens but on the consumption of vegetables year-round.
These are still early days in the project. Funding from the German Federal Ministry for Economic Cooperation and Development has enabled the project to be extended for an additional three years. Activities at village-level are ongoing with a focus now on sustaining new behaviours and achieving the ‘last mile’ in project villages before partners gradually phase out. This will take time and will require a continued multi-sector approach that is refined for the specific context of each country. In India, the focus will be on reducing women’s engagement in work outside the household and on home-based income-generating activities, as well as building skills to ensure sustainable dietary diversity and increased meal frequency for children. In Bangladesh, the focus will be on scaling up the programme through government systems. The creation of knowledge management platforms for experience sharing and the exchange of tools to minimise duplication and save time during scale-up of the Nutrition Smart Villages model is another focus area of the second phase, as well as the piloting of a mobile-based data collection and management system in Bangladesh that will share information with government institutions.
Further afield, evidence from this programme is being used to inform the implementation of the same model in other countries with high burdens of undernutrition. During this next phase, WHH is supporting implementation and scale up in Tajikistan, Afghanistan, Pakistan and Myanmar. Virtual workshops and ‘South to South’ exchange programmes are planned to support this effort as well as joint conferences with the SAARC agriculture centre5 in Dhaka involving representatives from all seven countries. Learnings will continue to be captured and shared.
For more information, please contact Sweta Banerjee at Sweta.banerjee@welthungerhilfe.de
1 SHG – Self-help groups (SHGs) are informal associations of people who choose to come together to find ways to improve their living conditions.
2 Participatory Learning for Action is a family of approaches, methods, attitudes, behaviours and relationships that enable and empower people to share, analyse and enhance their knowledge of their life and conditions and to plan, act, monitor, evaluate and reflect.
4 Tippy Tap is a hands-free device for hand washing that is specially designed for rural areas where there is no running water. It is operated by a foot lever and thus reduces the chance for the transmission of pathogens, as the user only touches a bar of soap suspended by a string.
5 SAARC Agriculture Centre is a South Asian Association for Regional Cooperation agency responsible for promoting Research and Development in agriculture in South Asian countries.
References
Ahmed, M and Suphachalasai, S (2014) Assessing the costs of climate change and adaptation in South Asia. Mandaluyong City, Philippines: Asian Development Bank. Access at: http://hdl.handle.net/11540/46
Development Initiatives (2020) 2020 Global Nutrition Report: Action on equity to end malnutrition. Bristol, UK: Development Initiatives. Accessed at: https://globalnutritionreport.org/0fb38d
International Institute for Population Sciences (IIPS) and ICF (2017) National Family Health Survey (NFHS-4), 2015-16: India. Mumbai: IIPS. Accessed at: https://dhsprogram.com/pubs/pdf/FR339/FR339.pdf
WHO/UNICEF (2017) Joint monitoring programme (JMP) for water supply and sanitation. https://washdata.org/