
Link NCA offers a new opportunity to study drivers of concurrent wasting and stunting (WaSt)
By Lenka Blanárová and Grace Heymsfield
Lenka Blanárová is Senior Nutrition Assessment Coordinator at Action Against Hunger UK. As a member of Link NCA Technical Unit she provides technical support to organisations implementing Link NCA studies worldwide.
Grace is a Registered Dietitian Nutritionist with five years of nutrition assessment and nutrition programming experience. She led a Link NCA study across five counties of Liberia and contributed at various degrees to Link NCA studies in Bangladesh, Haiti, Myanmar, Uganda and South Sudan.
The authors would like to acknowledge the following agencies for their engagement during the Link NCA exercise in Liberia, namely, the Liberia Wash Consortium, including Action Against Hunger, Concern Worldwide, Water Aid and Tearfund in Liberia with the technical support of their respective headquarters and the financial support of Irish Aid.
Location: Liberia
What we know: Link NCA (Nutrition Causal Analysis) is an established methodology for analysing the multi-causality of undernutrition to inform context-specific nutrition-sensitive programming.
What this article adds: This article summarises a recent Link NCA study covering five counties grouped into three regions in Liberia that extended its original research questions revolving around stunting to include analyses of concurrent wasting and stunting (WaSt). Logistic regression revealed significant associations between WaSt and younger age (<24 months) across all three regions. Further associations were apparent in one of three regions including episode(s) of diarrhoea during two weeks preceding the survey; child being taken care of by a non-immediate family member; medium to high score on reduced coping strategy index and/or caregivers’ perceived low level of social support. A child’s measles vaccination and caregiver’s perceived breastmilk sufficiency were protective factors in one region. Broader results revealed limited access to markets as the key root cause of stunting in this context. The authors conclude that analyses focusing purely on stunting would not allow for the design of interventions that address risk factors for WaSt for those who are at the highest risk of mortality. Shared risk factors for both stunting and WaSt should therefore be examined using Link NCAs in contexts with high burdens of wasting and stunting to better inform programme design.
Context
Wasting and stunting tend to be addressed as separate issues despite evidence of common causality and the fact that children may suffer simultaneously from both conditions (WaSt). Children with concurrent wasting and stunting may have comparable mortality risk to children with severe wasting only and they also tend to be more severely wasted than children who are only wasted (Wells et al, 2019). The heightened risk of mortality associated with WaSt means that further understanding of the aetiology, prevention, case-finding and treatment of children with WaSt, as well as the extent to which current interventions are reaching these children, is urgently required. Work on the mechanisms of the association between wasting and stunting on mortality may prove useful. Consideration should be given to encouraging the routine reporting of the prevalence of WaSt from nutritional anthropometry surveys, broader surveys (e.g. Multiple Indicator Cluster Surveys and Demographic and Health Surveys), surveillance systems and other nutrition information systems that collect and report on anthropometric data (Myatt et al, 2018).
As a part of extensive formative research to better understand context-specific causes of stunting and related behaviours in five counties in Liberia (Grand Bassa, Grand Cape Mount, Rural Montserrado, Rivercess and Sinoe), a Link NCA was carried out to identify and categorise risk factors for stunting across the study area. Specifically, the Link NCA aimed to describe interactions between identified risk factors, their seasonality and historical variations as well as most vulnerable groups among the population. The compiled evidence was used to develop a Theory of Change with actionable multisector recommendations to address identified risk factors, targeting most vulnerable communities, households, and children, to feed into programme design. A secondary research question emerged during the study’s qualitative inquiry, inspired by community members’ perception of malnutrition as wasting and not stunting. Therefore, the quantitative analyses conducted during the Link NCA were extended to wasting and concurrent wasting and stunting, to explore potential interactions of risk factors among multiple nutrition outcomes. In this article we focus on the extended WaSt analyses.
Box 1: About Link NCA
Link NCA (Nutrition Causal Analysis) is an established participatory and results-orientated methodology for analysing the multi-causality of undernutrition to inform context-specific nutrition-sensitive programming. The Link NCA methodology was developed to help researchers discover the prevalence and severity of undernutrition in a study population; statistical associations with a variety of individual and household indicators that depict the broader environment; causal pathways of undernutrition; changes in patterns of undernutrition over time and seasonally; risk factors and pathways likely to be the most modifiable by stakeholders; and recommendations for programming.
To answer these questions Link NCAs employ a mixed-methods approach, combining both qualitative and quantitative research methods, and draw conclusions from a synthesis of results. The Link NCA is carried out in the following five steps: preparatory phase; identification of hypothesised risk factors and pathways; community-level data collection; synthesis of results and building technical consensus; and communicating results and planning for a response.
For more information see https://www.linknca.org/
Methodology
The Link NCA is a mixed methods study, as described in Box 1. During the preparatory phase an in-depth literature review was undertaken to identify hypothesised risk factors for field testing during the qualitative inquiry and a quantitative survey. The second stage of this study, the qualitative inquiry, covered 10 sampled locations (two per county) across various livelihood zones and included 131 focus group discussions, 52 semi-structured interviews and 29 observations with over 1,300 participants. All qualitative data was recorded manually in a notebook and reproduced electronically at the end of each data collection period. The data was grouped by themes and analysed using qualitative content analysis methods.
The quantitative survey included the collection of anthropometric measurements of children under five years of age and 45 household indicators in 1,094 households across all five counties of the study zone, grouped into three regions, based on the 2016 Malaria Indicator Survey precedent.1 Household indicators included a range of standard and/or adapted indicators used in sectoral cross-sectional surveys, for example, Individual Dietary Diversity Score (IDDS),2 reduced Coping Strategy Index (rCSI)3 and others. The quantitative data was collected via an electronic questionnaire downloaded onto mobile devices. Paper anthropometry and mortality forms were maintained for verification before nightly upload of data onto the online platform KoBoToolbox. After final compilation, all data was exported in the form of an Excel spreadsheet and analysed with STATA software. The anthropometric data was analysed using ENA for SMART software (2011 version).4 The analyses included bivariate logistic and linear regressions (WaSt children vs. children with no anthropometric deficits). The final stage involved the synthesis and triangulation of data, which included design of causal pathways based on community perceptions, available scientific evidence and generated evidence.
Results
Communities visited during the qualitative inquiry did not perceive stunting as a medical condition and therefore discussions around its causal pathways were challenging. Despite a discrepancy of perceived severity of this form of malnutrition, there was a consensus that stunting differed from natural and normal shortness. A stunted child was described as being ‘tight’ in the body, meaning that he/she could not grow into his or her full height for age. ‘Tightness’ is differentiated from shortness if a child progressively falls further behind his/her peer’s growth. On the other hand, a wasted child was described as ‘dry’, meaning that his/her ribs protrude and his/her legs are ‘too skinny to carry him/her.’ Other nicknames for wasting tease at a child’s physical appearance, including dry and scaly like a ‘chameleon’ or ‘Mister Bone Chairman.’ Causes of wasting were directly or indirectly linked to perceived negligence of the child’s mother. A child is perceived at risk of becoming wasted if s/he ‘does not get food on time’, if s/he is not washed frequently enough and/or has frequent diarrhoea. Unlike general morbidities, a ‘dry’ child is more likely to be perceived to have been a victim of witchcraft.
Community aetiology of stunting roughly fell into three categories: hereditary, environmental and spiritual. The dominant belief is that a ‘tight’ child is short because his/her parents are short. A child could become stunted if s/he was not well taken care of in the home - this referred to both nutrition and household hygiene. A few community members identified pregnancy and lactation as influential times that could influence a child becoming or not becoming stunted, but this was typically recorded in areas that had been sensitised to the health benefits of breastmilk for child health. As was true for any other protracted undesirable situation (health, economic, etc.), a ‘very very tight’ child could have been vexed by witchcraft.
The overwhelming consensus was that boys were more vulnerable to stunting than girls. Boys were said to be greedy when breastfeeding. If their nutritional needs or preferences were not satisfied from infancy (meaning insufficient food, undesirable food, or both), they were believed to be frustrated and unable to grow.
A summary of terms used to refer to stunting and wasting are included in Table 1. It is important to note that terms used to refer to wasting implied a medical condition, while stunting was regarded as growth failure. No special terms were reported for a child who was concurrently wasted and stunted - the child could be called ‘tight and dry,’ or some combination of the below terms. A child who is ‘dry’ was identified as needing urgent treatment in the health facility, but no therapeutic treatment was implied for stunting.
Table 1: Local terms used to describe stunting and wasting
| Stunting | |
| Local term | Meaning |
| Tight | Short for age |
| Short butt AK-47 | Short for age |
| NGO – “Never grow old” | Unable to grow to potential |
| Small in the body | Short for age |
| Forever young | Looks younger than he should |
| Cornerstone | Never changing, never growing up5 |
| Little man | Small for age, with a face like an old man |
| Small man in the iron jacket | Very tight in the body; Increased severity |
| Lazy child | The baby is too weak to grow |
| Iron rock | A child who looks older than his age, but stooped like an elderly person |
| Wasting | |
| Dry | Dry skin, no fat in the body, child who is very sickly |
| Witch child | Child is a witch; the child is flying at night |
| Chameleon | Appearance like a lizard |
| Boney boney | Appearance like a dry boney fish |
| Malnourished | The child is very dry, weak, pure, dirty, dry and small in size |
| Win child | Poor birth spacing6 |
| Dirty child | The child is not cared for by his or her parent nor caregivers |
| Weaky weaky | Child who is sicker than other children |
| Mr. Bone or Bone Chairman | The child’s ribs and others bones of his/her body can be seen and counted |
| Skinny-winnie | The child’s legs and arms are very dry and his stomach is big |
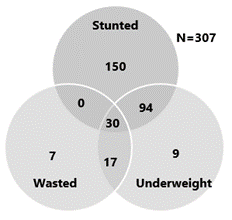
The quantitative survey revealed a prevalence of global chronic malnutrition (GCM) on the basis of height-for-age less than -2 z-scores (HAZ <-2) as above 30% in all three regions of the study, all classified as ‘very high’ according to WHO prevalence thresholds. Prevalence of global acute malnutrition (GAM) on the basis of weight-for-height z-score (WHZ <-2) ranged from 5.4% to 8.7%, classified as ‘medium’ according to the WHO thresholds. WaSt prevalence ranged from 3.4% to 4.1%. All children who were wasted and stunted were also underweight (30), as depicted in Figure 2. A majority of children who were stunted were not also underweight or wasted (150). Few children (17) were wasted, underweight, and not stunted.
Figure 2: Number of cases by anthropometric deficiency (excluding children with no anthropometric deficiencies)
Logistic regressions, by region, revealed significant associations between concurrent wasting and stunting and the indicators presented in Table 2. Indicators are highlighted in orange if exposure is a risk factor significantly associated with higher odds of WaSt and green if exposure is a protective factor significantly associated with lower odds of WaSt (p <0.05). A child who is less than 24 months of age was more likely to be WaSt. This was true across all three regions of the study. Regional variations in other risk factors should be interpreted with caution, as correlations were limited by the small percentage of children with WaSt and should not be considered relevant to only one region without further investigation. Such risk factors include the child having episode(s) of diarrhoea during the two weeks preceding the survey, the child being taken care of by a non-immediate family member, medium to high reduced coping strategy index (rCSI) and/or caregiver’s perceived low level of social support. A child’s measles vaccination and caregiver’s perceived breastmilk sufficiency came out as protective factors in Region III. The analyses showed almost no overlap of risk factors for stunting and WaSt apart from the mining/concession livelihood zone being a risk factor for wasting and stunting and potentially for WaSt. Some risk factors, including age group <24 months, measles vaccination and rCSI were associated with both wasting and WaSt but not stunting.
Table 2: Select indicators’ association with WaSt

Broader results revealed that the dominant overarching pathway to stunting in this context took roots in limited access to markets, which appear to exacerbate a variety of household factors, including personal and environmental hygiene, as well as consumption of a diverse and nutritious diet. The study also substantiated evidence regarding the role of women’s nutritional status and social support in the health and wellbeing of their child. The nutritional status of women, assessed using mid-upper arm circumference (MUAC), was significantly linked with a child’s HAZ score. In agricultural livelihoods zones, where access to resources is intrinsically linked with the availability of external support, children of mothers with perceived low levels of such support and who were not part of external support groups, were potentially at a greater risk of stunting.
Discussion and conclusion
The Link NCA study in Liberia was completed as part of a three-assessment package of formative research, which informed a project design process for the Liberia WASH Consortium (LWC), including Action Against Hunger, Concern Worldwide and Water Aid. The Link NCA study yielded meaningful evidence regarding stunting and WaSt that informed the design of a holistic intervention targeting both forms of undernutrition. Analyses focusing purely on stunting would not necessarily allow for a design of interventions encompassing concurrent forms of undernutrition, for example by addressing mothers’ breastmilk production, which the analyses found to be solely associated with WaSt.
Due to the multifaceted nature of findings, and facilitation of the proposal development by an external partner, consortium partners were led to design a novel project and not repeat status quo programming, putting children at the highest risk of mortality (WaSt) at the heart of programme design. On the basis of this experience, we recommend that contexts with high stunting and wasting burdens use Link NCA studies to explore risk factors for WaSt to ensure that programmatic recommendations are tailored to address the needs of children at most risk, according to the specificities of the intervention zone.
It must be acknowledged that this Link NCA study did not substantiate evidence to suggest effects on linear growth slowing as a child’s wasting progresses, or vice versa. The current research design is limited to a snapshot of a child’s nutritional status at the time of the data collection as opposed to longitudinal studies, which collect the relevant data points over an extended period of time. In addition, while stunting is less influenced by seasonality than wasting, available cross-sectional data did not substantiate potential seasonal stresses that influence growth faltering, whether that be wasting or stunting. Therefore, it is important to consider an integration of longitudinal evidence in the structuring of causal pathways, especially regarding the influence of wasting on stunting and vice versa.
More details on the methodology and findings can be found in the full report which is available from https://linknca.org/etude/grand_bassa_great_cape_mount_rural_montserrado_rivercess_and_-sinoe_counties.htm
For more information, please contact Link NCA Technical Unit at Action Against Hunger UK/ Action Against Hunger France at Link-nca@actioncontrelafaim.org
1 Region 1 covered Grand Cape Mount Country, Region 2 Rural Montserrado and Grand Bassa Counties and Region 3 Rivercess and Sinoe Counties.
2 Indicators for assessing infant and young child feeding practices Part 2 Measurement. Available at: http://www.unicef.org/nutrition/files/IYCF_Indicators_part_II_measurement.pdf
3 Maxwell, Daniel, Jennifer Coates, and Bapu Vaitla (2013). How Do Different Indicators of Household Food Security Compare? Empirical Evidence from Tigray. Feinstein International Center, Tufts University: Medford, USA.
4 Children with missing or flagged WHZ and HAZ information were dropped; WHO 2016 flags applied.
5 The child is the oldest of all the children in the community but he/she is very short and small.
6 The child was ‘won’ by parents by having sex too soon after the preceding baby.
References
Wells J.C.K., Briend A., Boyd E., Berkley J.A., Hall A., Isanaka S., et al. Beyond wasted and stunted – a major shift to fight child undernutrition. Lancet Child & Adolescent Health, Online, September 11, 2019
Myatt, M. et al. Children who are both wasted and stunted are also underweight and have a high risk of death: a descriptive epidemiology of multiple anthropometric deficits using data from 51 countries. Archives of Public Health (2018) 76:28, https://doi.org/10.1186/s13690-018-0277-1