
Prioritising Emergency Response Preparedness: Global Nutrition Cluster supports countries to plan for potential humanitarian crises
Anteneh Gebremichael Dobamo is a Deputy Global Nutrition Cluster Coordinator and leads the operational support team at the Global Nutrition Cluster (GNC).
Faith Nzioka is a Nutrition Cluster Coordinator on the GNC’s Rapid Response Team.
Briony Stevens serves on the Coordination Helpdesk at the GNC.
The authors would like to acknowledge the leadership of the GNC Coordination Team in identifying and addressing preparedness at a country-level and the work by all Nutrition Cluster and Sector Coordination teams and their partners in this respective area of work. In particular, the authors thank Stefano Fedele, the GNC Coordinator, Maguette Ndiaye, UNICEF Emergency Specialist, Anteneh Dobamo, GNC Operational Support Team Lead, Elena Gonzalez, Advocacy Specialist, Magnat Kavuna, GNC Rapid Response Team Information Management Officer, Shabib AlQobati, GNC Information Management Specialist, Annabel Judith Hodge, GNC Communications Specialist, all nutrition coordination mechanisms that have participated in the GNC-led Emergency Response Preparedness efforts and, most importantly, to all the communities that we are here to support and that have been involved in various preparedness initiatives to date, the authors thank you for your invaluable contributions.
The information in this document expresses the authors’ personal views and opinions and does not necessarily represent UNICEF’s position.
Background
The 2022 Humanitarian Overview estimates that over 274 million people will need humanitarian assistance and protection in 2022, the highest annual figure recorded to date. The magnitude, frequency and duration of crises are rising due to climate change, conflict and the COVID-19 pandemic. Humanitarian emergencies exacerbate nutritional risks and often increase wasting and micronutrient deficiencies in vulnerable population groups including women, children, adolescents, people with disabilities and the elderly.
Over the last few decades, the global humanitarian agenda and policies have increasingly focused on resilience to ensure people, communities and countries are best prepared to anticipate, manage and recover from shocks for sustainable long-term progress. In 2015, the Inter-Agency Standing Committee (IASC) developed the Emergency Response Preparedness (ERP) approach to improve the humanitarian system's readiness to respond to crises (see Box 1). The ERP approach consists of three key elements including risk analysis, preparedness actions and contingency planning and closely aligns with the Humanitarian Programme Cycle, if activated. With the increasing frequency and magnitude of emergencies that potentially affect every country, coupled with the global COVID-19 pandemic and the related response efforts, adopting emergency preparedness for a potential nutrition response has never been more relevant.
Prioritising ERP
The new Global Nutrition Cluster (GNC) Strategy (2022-2025) highlights a shift in focus from providing operational and technical support during Nutrition in Emergencies (NiE) response and recovery phases to including support for preparedness for humanitarian crises and covering the protection of the nutrition status of people at risk during situations of fragility.
Emergency preparedness for nutrition can be conducted at various levels and involves a wide range of actors such as aid agencies, national institutions and organisations, inter-sectoral teams and the private sector. The ERP approach enables country teams in low, medium to high-risk contexts to identify and unpack potential response activities and to implement these activities as well as to identify and prioritise gaps in preparedness. Examples of preparedness actions for nutrition include ensuring that a dedicated nutrition coordination mechanism is established, the rationale and methods for needs assessment and analysis are understood by partners and that capacity mapping is performed and regularly updated.
However, not every country routinely conducts a preparedness exercise with many completed on an ad hoc basis. The GNC identified the need to prioritise ERP following the 2020 Cluster Coordination Performance Monitoring exercise conducted with 20 countries and through discussions with country-level coordination teams. Most countries did not have a preparedness mechanism in place – and for those that did, the plans were either not comprehensive or did not follow standard guidelines. As a result of this exercise and in line with the new strategy, ERP has been made a priority for the global-level GNC operational support team.
ERP approach
In practical terms, the ERP approach is led by the resident/humanitarian coordinator managed by the humanitarian country team and supported by the inter-cluster/sector coordination group and clusters/sectors. As with the humanitarian needs overview (HNO)/humanitarian response plan (HRP) approach, each cluster is expected to contribute to the United Nations Office for the Coordination of Humanitarian Affairs (OCHA)-led process and has its own unique role. However, unlike the HNO and HRP approaches, the ERP approach offers greater flexibility. For example, preparedness may not be initiated by OCHA or the inter-agency preparedness response may not adequately address nutrition. In these contexts, the Nutrition Cluster may decide to conduct its own ERP exercise, bearing in mind that governments hold the primary responsibility for providing humanitarian assistance, with the ERP providing guidance on how the international humanitarian community can support and complement national action.
The aim of ERP is to identify the most appropriate response activities for a given crisis and ensure that operational readiness is in place to respond quickly and effectively in the first four to six weeks of an emergency. However, this is not an isolated approach and preparedness is an integral part of the Humanitarian Programme Cycle process. Additionally, conducting an ERP exercise identifies the additional risks not captured by the HNO or HRP approaches. If an emergency does occur, this may result in the amendment of the HRP or an annexed response plan as seen in recent examples with Myanmar and Afghanistan.
Key steps in the ERP process
Figure 1: Sequencing of ERP components: risk analysis and monitoring, minimum preparedness and advance preparedness actions
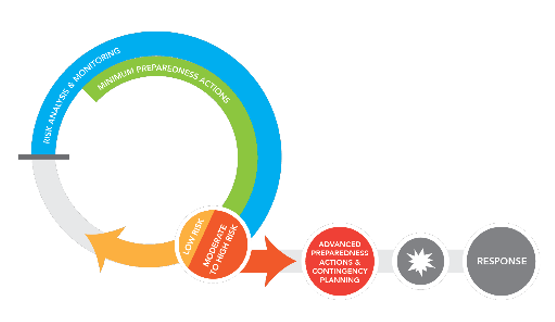
1. Risk analysis & monitoring
The risk analysis identifies the factors that could trigger a crisis and ranks these in terms of impact and likelihood with those identified as medium or high requiring contingency planning. Risk analysis is integrated into the HNO process and draws from the expertise of a wide range of partners including aid agencies, national institutions and organisations and independent experts. A clear and common understanding of the risks faced by a country is fundamental to the ERP process.
Risk monitoring provides early warning of emerging risks which allows for early action. Monitoring should be indicator based with at least one person or entity tasked with monitoring the indicators for each hazard on a scheduled basis using updated information. Relevant nutrition outcome indicators and key contributing indicators should be used. For example, in a drought disaster scenario, trends on the prevalence of wasting and food consumption scores from surveillance systems can be included in the monitoring system. However, in a sudden onset disaster scenario such as flooding, monitoring information can be obtained from the Global Flood Awareness System and national meteorological forecasts which is usually communicated through inter-agency platforms.
2. Contingency planning1
A contingency plan is required for risks identified as medium or high through the risk analysis (which fall outside of any existing HRP). This plan provides an overview of humanitarian partners’ capacities and approaches to meet the immediate needs of affected communities in the first four to six weeks of the response and prioritises preparedness actions through a workplan. In general, contingency plans consist of six main sections including: (1) a situation and risk analysis (including gender and diversity analysis); (2) a response strategy; (3) operational delivery; (4) coordination, management and operational support arrangements; (5) preparedness gaps and actions; and (6) funding requirements. The contingency plan should be updated and modified when more specific information becomes available and build upon the relevant preparedness actions discussed below. The most common contingency measures for the Nutrition Cluster include:
- Scaling up/strengthening coordination at local level
- Scaling up programmes to cover new areas; for example, a new outpatient therapeutic programme may be established in health centres not previously providing this service and hospital bed capacity for inpatient care may be increased.
- Scaling up nutrition assessments and referral screening; for example, increasing the frequency of mid-upper arm circumference (MUAC) screening to allow for the early detection of new cases; planning SMART surveys in high-risk areas; ensuring systematic screening at health consultations and establishing/expanding mothers’ MUAC for diagnosis and referral of malnutrition.
- Early procurement of therapeutic food, drugs, anthropometric materials and supplies needed for nutrition programmes.
- Pre-positioning of food and supplies in regional, district or point-of-delivery facilities.
- Contracting of vendors and service providers for the provision of cash or vouchers. Cash and voucher assistance allows recipients to purchase locally available goods (nutritious foods, sanitation and hygiene items, water) and can facilitate access to health/nutrition services by covering direct costs (e.g., consultation fees, medication) and indirect costs (e.g., transportation, accommodation).
- Training/retraining of staff based on identified needs and gaps. Staff may include management staff (e.g., Ministry of Health nutrition focal points at district level), healthcare providers (e.g., nurses, doctors), community health workers and support personnel (e.g., distribution agents, Information Management Officer, etc.).
If the emergency occurs, the contingency plan should feed into the flash appeal for funding and speed up its allocation.
Afghanistan example
While Afghanistan has an active Humanitarian Programme Cycle, contingency planning processes were completed prior to the withdrawal of US troops to ensure an advanced level of readiness to respond to the humanitarian consequences due to the potential armed conflict. The contingency planning processes included the identification and implementation of several preparedness actions from strengthening coordination mechanisms at national and sub-national levels to increasing the frequency of monitoring trends of wasting.
3. Preparedness actions
Minimum Preparedness Actions (MPAs) represent a set of core preparedness activities that need to be undertaken by low-risk countries to achieve positive outcomes in the initial phase of the emergency response. MPAs focus on practical actions to improve response, accountability and predictability. They also promote more effective coordination between humanitarian actors, considering the perspectives of affected populations through situation (baseline) and needs analysis which includes the collection of sex- and age-disaggregated data. MPAs are particularly useful for contexts where humanitarian capacity is limited and where any potential response would rely on external capacity.
Advanced Preparedness Actions (APAs) are designed to guide the nutrition coordination team towards an advanced level of readiness to respond to a specific risk. Unlike MPAs, APAs are risk-specific and build on the existing MPAs.
Countries with ongoing emergencies, or with medium to high risks, should have a workplan which consists of both minimum and advanced preparedness actions which respond to specific risks – most countries supported by the GNC will fall into this category. This mixed basket is required to ensure an advanced level of readiness to respond to the identified risks.
Preparedness support for countries
The GNC is currently developing a series of resources and tools to better support country coordination teams with preparedness. The first step was the publication of the GNC Preparedness Guidance2 which aims to help country-level Nutrition Clusters, nutrition sector coordination and nutrition working groups to strengthen collective preparedness towards the effective protection of the nutritional status of populations. The document primarily focuses on preparedness actions and touches on the risk analysis process and contingency planning (it is due to be updated to take into account IASC 2020 Guidance).
In 2021, two webinars on ERP were conducted by the GNC, an introduction to ERP Planning for Nutrition Coordination Mechanisms,3 where a pilot was launched to set up ERP platforms in 10 countries, and an ERP Satellite event4 at the GNC Annual Meeting. In addition, the GNC has developed online tools5 and a workshop package6 to support countries in their ERP approach process and these will be updated following the pilot and lessons learned workshop. Furthermore, the GNC has developed an e-learning module on the ERP approach7 and is currently developing additional modules specifically on the use of the GNC ERP tools.
Myanmar: An ERP Case Study
Myanmar was the first country to finalise its ERP process using the GNC’s guidelines and tools alongside deployment support from the Technical Support Team’s Nutrition Cluster Coordinator. This was achieved against a backdrop of an evolving humanitarian crisis in which the country’s military forces seized power from the government on 1 February 2021, just weeks after Myanmar finalised its 2021 HRP. The operating environment in the country has become more complex as nutrition partners work to reach affected populations while attempting not to engage with the de facto authorities in a way that legitimises them.
Myanmar’s nutrition sector organised a three-day ERP workshop in April 2021 to mobilise assistance to those affected by the humanitarian crisis. The workshop was attended by over 70 stakeholders including non-governmental organisations (NGOs), international NGOs and the private sector with the active participation of the Scaling Up Nutrition Movement platform and networks although government actors were not involved due to the coup. The main aims were to identify various hazards in different parts of the country that had not been included in the HRP 2021 and to develop a contingency plan. High-risk hazards were confirmed as armed conflict and floods with COVID-19 classified as medium risk. All three risks were included in the contingency plan which included agreed priority interventions and geographical areas for preparedness actions.
Table 1. Draft Response Plan and Preparedness Priorities April 2021
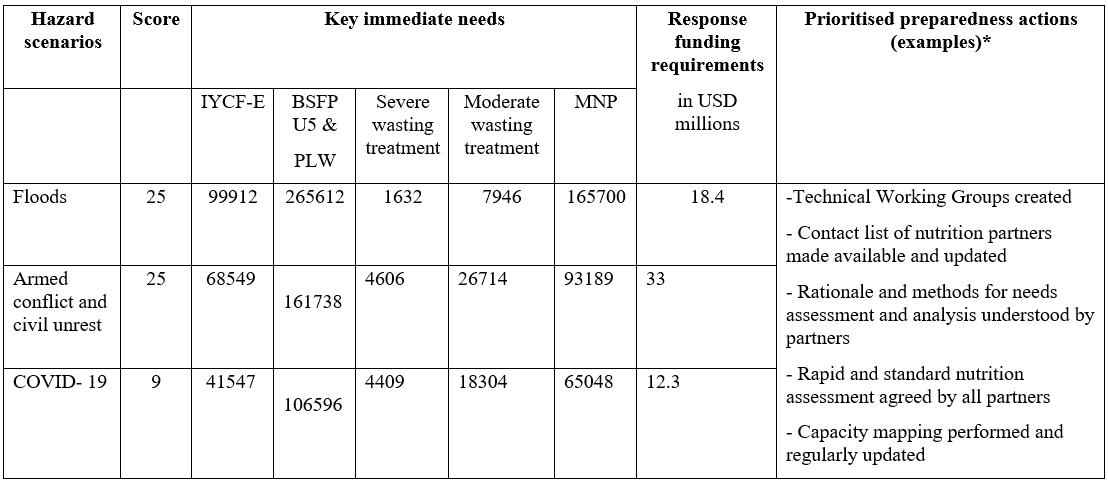 Infant and Young Child Feeding in Emergencies (IYCF-E)Blanket Supplementary Feeding Program for Children <5 Years and Pregnant and Lactating Women (BSFP U5 & PLW)
Infant and Young Child Feeding in Emergencies (IYCF-E)Blanket Supplementary Feeding Program for Children <5 Years and Pregnant and Lactating Women (BSFP U5 & PLW)
Multiple Micronutrient Powder (MNP)
*The preparedness actions are relevant for the three hazards, however, each scenario required specific anticipatory actions.
The timing of the ERP process was challenging as it took place during the peak of the armed conflict when partners were expected to provide planning for a response rather than for preparedness. However, the ERP workshop did present an opportunity for nutrition partners to ‘think on their feet’ and agree on some immediate actions. One outcome was the establishment of technical working groups for the integrated management of acute malnutrition and infant and young child feeding in emergencies and assessments for partners to be able to quickly operate, scale up and deliver life-saving activities in the current context. While humanitarian response efforts were timely in areas where there was an established operational NiE presence, response efforts in other geographical areas were slow primarily due to financial, human and programmatic resources. The Myanmar Preparedness Action Workplan8 has now been developed with the funding requirements updated as new information is received.
OCHA Myanmar activated an ERP working group with the participation of all sectors and clusters but ERP processes are at different stages for different actors. The nutrition sector was the first to complete the ERP process using the new IASC guidelines and this has been instrumental to ongoing OCHA processes especially the HRP 2021 revision and to mobilising funding for Myanmar humanitarian projects.
Remaining challenges
Making ERP a priority for all stakeholders, including donors and academia, remains a challenge and many countries are still prioritising the response to humanitarian crises. Although countries are becoming more fragile due to the increased frequency and intensity of natural disasters and an increase in the complexity of conflicts, humanitarian coordination teams at country level are still not fully aware of ERP processes and there is limited funding for the effective implementation of preparedness actions. The need to strengthen capacity of humanitarian actors and to continuously update ERP processes are key lessons learned to prepare well for the future. This could be partially achieved through better addressing ERP including early actions in the Humanitarian Programme Cycle and addressing it as an annual output alongside the HNO, the HRP and the Cluster Performance Monitoring exercise.
GNC Coordination Team efforts, as outlined under the preparedness support for countries and the next steps below, seek to ensure harmonised ERP tools and processes across country clusters/sectors. This is now being achieved in those countries that are taking part in the piloting phase as seen in the Myanmar example above. There is also a need for a more standardised approach since methods can vary between government-level approaches and those formulated by clusters in conjunction with OCHA. It is important to address how to avoid duplicated efforts and to ensure everyone is ‘on the same page’ when it comes to ERP.
Next steps
The GNC is expanding its guidance on the ERP process by conducting a lessons learned workshop with those countries that participated in the GNC ERP guidance piloting, updating all guidance based on the findings of this pilot, finalising an ERP checklist and building capacity through the development of two additional e-learning modules (Introduction to GNC ERP tools and Developing a contingency plan with partners) and organising regional-level training for Nutrition Cluster Coordinators. Many of the key ERP elements developed by the GNC can be used to expand work that has already taken place at country level on preparedness while aligning with the methodology implemented by OCHA and building on preparedness efforts led by other actors including local authorities.
In addition to Myanmar, other countries that participated in the piloting of the new GNC guidance are at various stages of the ERP process. These include Afghanistan, Bangladesh, Niger, Sudan, DR Congo, Ethiopia, Lebanon, South Sudan, Yemen and Somalia. Feedback and lessons learned from these countries will be used for the subsequent revision of the GNC ERP guidance.
For more information, please contact Anteneh Dobamo at adobamo@unicef.org
1 According to latest IASC guidance (under publication), contingency planning is the second element of the ERP Approach.
2 https://www.nutritioncluster.net/resource_GNC_preparedness_guidelines
3 https://www.nutritioncluster.net/event/GNC_ERP_webinar
4 https://www.nutritioncluster.net/node/27716
5 https://ee.humanitarianresponse.info/x/0G6SQrqw
6 Available on request to the GNC.
7 https://agora.unicef.org/course/info.php?id=33238
8 https://www.nutritioncluster.net/preparedness