
Cambodia: Impacts of the nutrition transition on urban and rural mothers and children
Hillary Fry Registered Dietitian for Northern Health, Kitimat, Canada
Sanne Sigh Advisor for the Multisectoral Food and Nutrition Security (MUSEFO) project, Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ), Phnom Penh, Cambodia
What we know: The nutrition transition – which stems from economic and related demographic changes – is characterised by changes in food environments and increasing access to highly processed foods, which can alter the traditional dietary patterns of mothers and children.
What this adds: This article provides an exploratory comparison of the ongoing nutrition transition in urban and rural Cambodia among caregivers and their children. This provides important insights for Cambodian policymakers and programmes to optimally address these challenges and ensure the health and livelihoods of caregivers, their children, and the country.
The nutrition transition
In low- and middle-income countries (LMICs) such as Cambodia the transition from food environments based on home production to those high in processed and mass-produced foods is particularly impactful. The traditional diet in Cambodia typically contains rice, fruits, vegetables, and low-fat protein sources, but has shifted to include more ultra-processed foods. Snack food and sugar-sweetened beverage consumption has risen, particularly among children (National Institute of Statistics, 2022). While undernutrition remains a challenge, rises in diabetes and other non-communicable diseases are already emerging (Kulikov et al., 2019).
“Very little is known about the ongoing nutrition transition in Cambodia. Research investigating the impacts of the changing food environment on food gathering and purchasing remains scarce.”
Recognising this gap, the Multisectoral Food and Nutrition Security (MUSEFO) project (Box 1) conducted a study exploring the effects of the ongoing nutrition transition on purchasing and consumption patterns among Cambodian caregivers and children. This article provides preliminary results from the Nutrition Transition and Food Environment Study, investigating both urban and rural areas in Cambodia.
Box 1: Data sourcing and ethical approvalOur data was collected within the MUSEFO project, which is a part of the Global Programme ‘Food and Nutrition Security, Enhanced Resilience’ under the Special Initiative ‘Transformation of Agricultural and Food Systems – For A Life Free of Hunger’ run by the German Federal Ministry for Economic Cooperation and Development. The project is owned by the Council for Agricultural and Rural Development, funded by the German Federal Ministry for Economic Cooperation and Development, and implemented by GIZ since 2015. The main outcomes of MUSEFO are to improve the dietary diversity of women of reproductive age, particularly pregnant and lactating women, and improve the minimal acceptable diet of 6–24-month-old children. The National Ethical Committee for Health Research approved the study by the Cambodian Ministry of Health on 27 November 2022 (Approval No. 039). Consent was received from participants before any data were collected. Participants could withdraw their consent or refrain from answering questions without any influence on the services or support they received. After the survey, participants were compensated with a krama, a traditional garment that can be used for multiple purposes. |
Our study
We used a mixed-methods design approach combining quantitative and qualitative observational data. This article presents the quantitative results from the household survey conducted between January and August 2021. Participants were from 68 villages across one urban (Phnom Penh) and two rural (Kampong Thom and Kampot) provinces of Cambodia. Participants were mothers or caregivers of a child aged 6–59 months.
To include a broader sample of the Cambodian population and to allow analysis of urban/rural differences, data presented here were gathered from: 1) beneficiary families of the MUSEFO project, who had received nutrition and basic hygiene education using the care group approach combined with nutrition counselling during home visits, living in rural Kampong Thom and Kampot; and 2) a random sample of families who were not beneficiaries of the project, living in Kampot, Kampong Thom, and Phnom Penh. Beneficiaries were recruited through the project and non-beneficiaries by purposive sampling in target provinces.
All study participants completed a questionnaire on a tablet, with reading and comprehension assistance from a research assistant, exploring food perceptions, gathering and purchasing practices, and the Cambodian adaptation of the Diet Quality Questionnaire (DQ-Q) developed by the Global Diet Quality Project (2023), for both caregiver and child. From the DQ-Q, a Global Diet Recommendation (GDR) ‘healthy’ score was calculated, measuring the consumption of healthy foods (e.g., fruits and vegetables) and a GDR ‘limit’ score measuring consumption of foods to limit or avoid (e.g., sugar-sweetened beverages). In both cases, a higher score indicates greater consumption. The DQ-Q is a globally applicable, valid, and reliable tool created to enable population-level diet quality monitoring (Herforth et al., 2020).
Descriptive data are presented as n (%) or mean (standard deviation). Sociodemographic factors were analysed using Chi-square with Bonferroni post hoc analysis for categorical variables, while t-tests were used for continuous variables. A p-value of <0.05 was considered statistically significant. Non-parametric continuous data (e.g., GDR scores) were analysed using the Mann-Whitney U test. GDR-Limit and GDR-healthy scores were calculated following directions described by the Global Diet Quality Project (Herforth et al., 2020). GDR-limit scores were analysed by various continuous variables using Pearson correlation and by categorical variables using t-tests. The higher the GDR-limit score, the more food is consumed in this category, and the less likely healthy eating recommendations are met.
Results
Study sample
This sample included 1,033 caregivers (97% female). Most participants (92%) were partnered and had low levels of education (7.5±4.2 years). Primary caregivers were mothers (82%), grandmothers (15%), fathers (2%), and others (2%). Participants had an average age of 34.0±10.6 years, which is older than the average age of mothers in Cambodia and with wide variation due to the inclusion of grandparents. Each of these factors was relatively consistent across rural and urban groups.
Significantly more respondents (p<0.001) living in urban areas were employed full-time (13%) and owned a small business (30%) compared to those in rural areas, at 3% and 22%, respectively (Table 1). Urban households reported a significantly higher monthly income of $708.72 compared to $339.30 among rural households. However, income also showed large variability within urban and rural populations. More participants lived in rural areas (n=757) compared to urban settings (n=276) in this study. This population was not balanced but does reflect Cambodia's urban/rural distribution, as it is still a predominantly rural country. None of the urban participants (Phnom Penh) in this analysis were from the beneficiary group.
Table 1: Differences in study populations
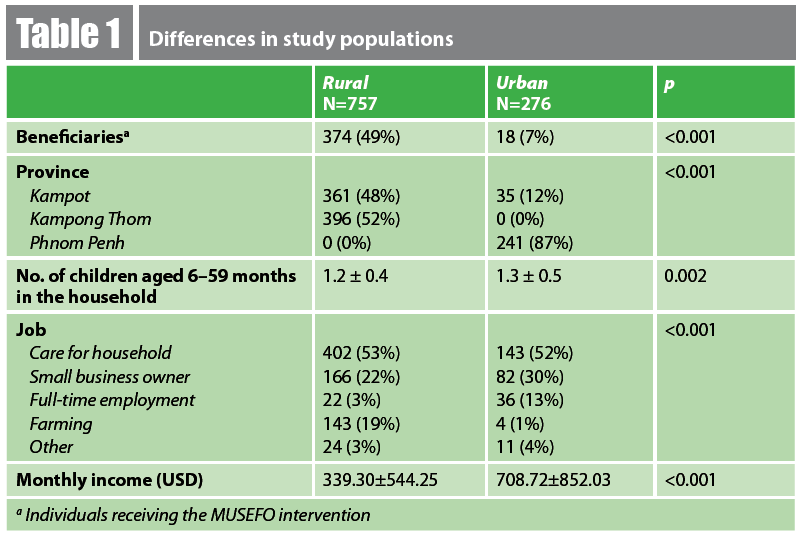
a Individuals receiving the MUSEFO intervention
Key findings
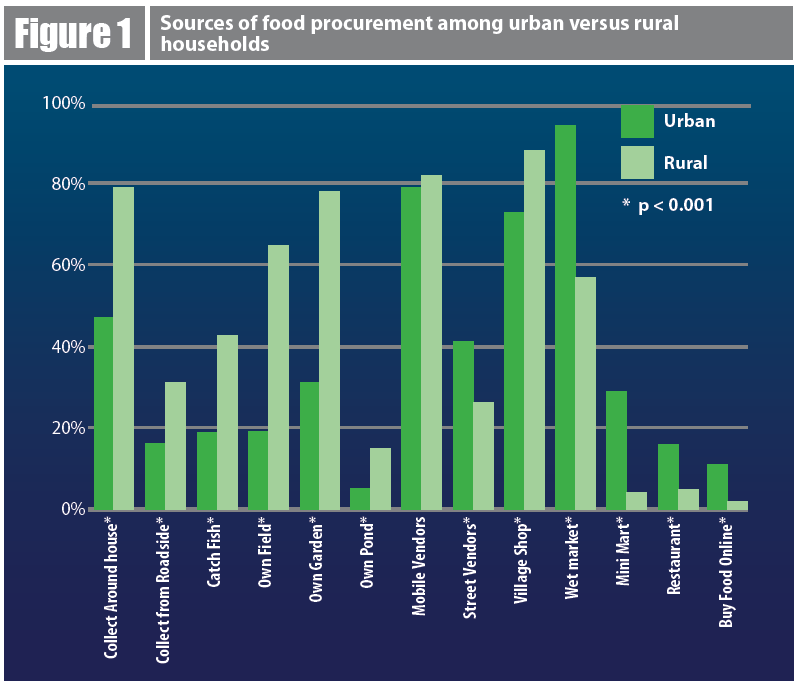
A significantly higher portion of rural versus urban households procured their food from their own or nearby sources such as their own fields (65%; 19%), gardens (78%; 31%), ponds (15%; 5%), or fishing in a nearby river/ocean (43%; 19%) (Figure 1). Significantly more urban households sourced their food from establishments such as street vendors (41%; 26%), wet markets (94%; 57%), mini marts (29%; 4%), restaurants (16%; 5%), and online (11%; 2%). Mobile vendors2 were an equally common food source for rural and urban households (82%; 79%).
Figure 1: Sources of food procurement among urban versus rural households
GDR-limit scores were significantly positively correlated with household income for both caregivers and children among rural participants – as household income increased, consumption of foods in the ‘limit’ category also increased (Table 2). Rural caregivers and children from households identified as earning below the poverty line had significantly lower GDR-limit scores. This may provide evidence that disposable income is more likely to be allotted to snacks and sweets or, in the context of Cambodia’s rates of malnutrition, poverty could simply indicate lower overall intake of all foods. This relationship was also not seen for urban households above or below the poverty line, reinforcing the hypothesis that wealth may have less of an effect due to already greater access/exposure to various food sources – particularly unhealthy food sources brought with a nutrition transition.
Further analysis showed that GDR-limit scores were significantly (p<0.001) positively correlated with GDR-healthy scores among both caregivers (0.233) and children (0.297) for both rural and urban participants. This suggests that less nutritious foods may not replace nutritious foods in this setting but are instead consumed in addition to healthier foods. Regardless, our data show significant consumption of energy dense foods with high sugar and salt content among Cambodian caregivers and children, which warrants concern for future rates of non-communicable diseases.
Table 2: GDR-limit scores of urban and rural caregivers and children
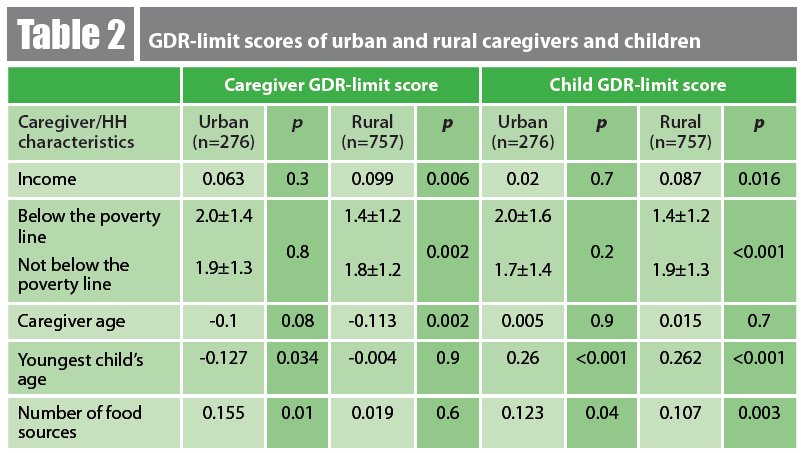
GDR-limit scores were significantly positively associated with the number of food sources commonly used by the household among urban caregivers and children, and rural children. However, this was not true for rural caregivers (Table 2). The importance of dietary diversity is demonstrated here – greater variety in food sources likely means greater variety in food, which is captured in the GDR-limit score calculations. A similar pattern of greater variety in urban areas and less variety among rural participants has been seen mid-nutrition transition in other Southeast Asian countries (Lipoeto et al., 2012).
Caregiver age was only observed to be significant for rural caregiver GDR-limit scores, but not for urban caregiver GDR-limit scores or child GDR-limit scores in either setting. This may indicate that rural caregivers are younger and have unhealthy food preferences, have less experience in selecting appropriate foods for themselves, and/or exhibit less traditional dietary influence.
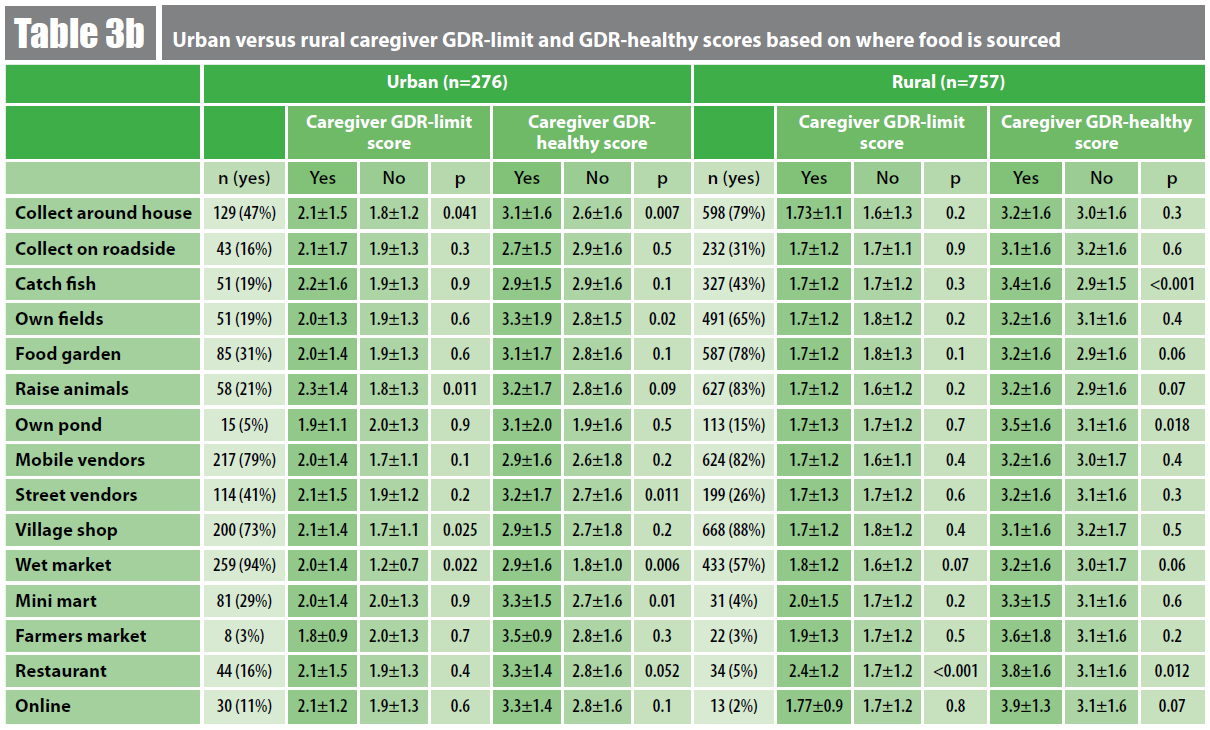
Although some differences were seen among rural caregivers and children, scores were not as impacted by the source of food as urban participants, whose scores were significantly associated with where they tend to procure food (Table 3). Among our urban participants, wet markets, raising animals, and collecting food from around the house all were associated with higher GDR-limit and GDR-healthy scores. This is likely explained by the source’s provision of food in both the limit and healthy categories (e.g., beef from the limit category; chicken from the healthy category). Catching fish and owning a pond were both associated with higher GDR-healthy scores among rural children and caregivers, as both increase access to foods included in the ‘healthy’ category, such as fish.
Table 3a: Urban and rural child GDR-limit and GDR-healthy scores based on where food is sourced
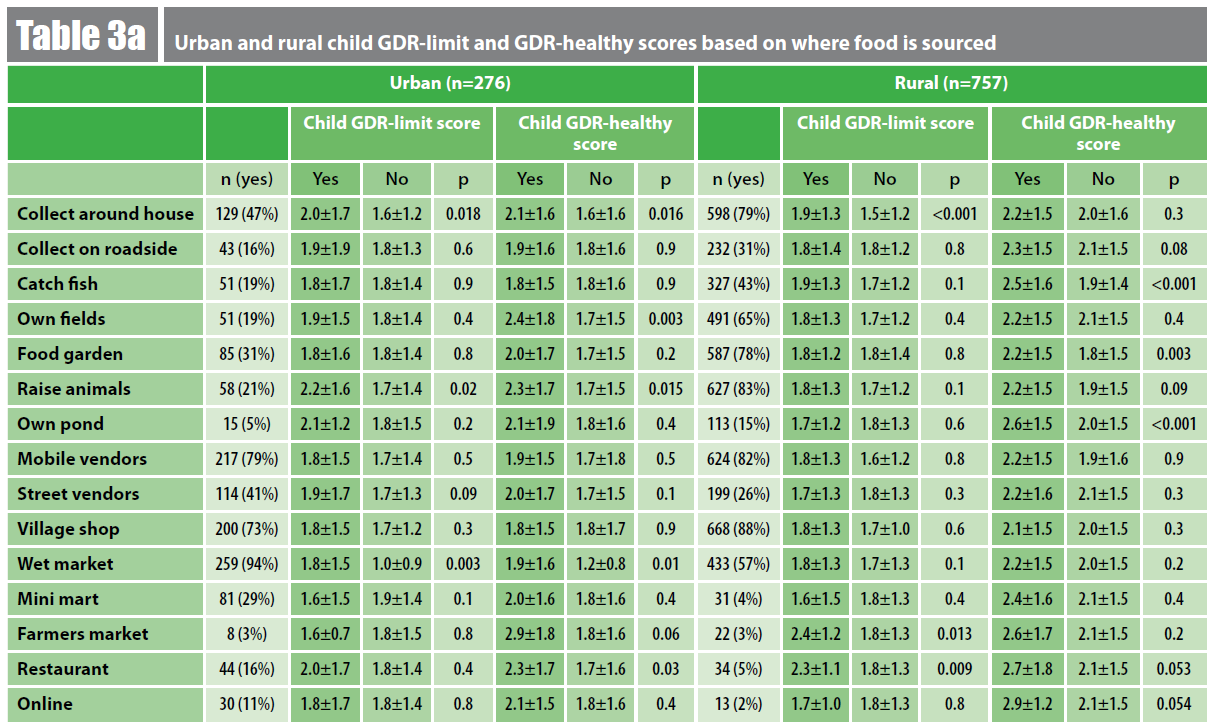
Table 3b: Urban versus rural caregiver GDR-limit and GDR-healthy scores based on where food is sourced
Conclusion and lessons learned
A nutrition transition occurs alongside urbanisation. Urban areas in Cambodia have greater access to supermarkets and modern retailers, exposure to marketing, and a changing workforce with higher household incomes that support the purchase of convenience and ultra-processed foods (Consortium for Improving Complementary Foods in Southeast Asia, 2023). This was reflected in our results, with urban participants identifying similar food sources and less reliance on household production of food. While rural households rely more on traditional food sources, mobile vendors – where salty snacks, sweet treats, and ultra-processed foods tend to be sold – were significant sources of food, although they were not associated with a higher GDR-limit score in this sample.
The diet of urban households included in this study was more often related to, and potentially influenced by, where food is sourced. Diet scores in rural households was significantly associated with income. With low incomes in rural areas and more limited choices in regard to food sources, it would be expected that income would have a significant influence on diet.
Overall, GDR-limit scores increased as GDR-healthy scores increased in both urban and rural participants. The general concern that, during a nutrition transition, salty snacks, sugar-sweetened beverages, and other ultra-processed foods replace nutrient-dense foods has not happened. Instead, it appears that a greater overall intake includes all foods among this sample. It is still likely, though, that this impacts how income is spent and could still contribute to micronutrient deficiencies (Bose et al., 2018). Further, with already rising rates of non-communicable diseases such as diabetes in Cambodia, the described intake of highly processed, energy-dense foods high in sugar and salt, particularly among children, raises concern regarding the future health of Cambodians (National Institute of Statistics, 2022).
One limitation of this study is the potential for observation bias, given that survey questions were administered with assistance from Khmer-speaking research assistants. These research assistants may have introduced their own biases by mistranslating participant answers and/or their presence may have affected participant response due to social norms. However, this did improve study accessibility for those who could not read or write, which in turn minimised selection bias, as well as reducing any translation errors. Participants were not informed about their compensation with a Krama prior to the interview, also reducing selection bias. A further limitation of the study is the mixed sample of beneficiaries and non-beneficiaries of the MUSEFO project and an uneven distribution of these within the urban and rural settings. The beneficiaries had received education on basic hygiene, home farming, and nutrition. However, the inclusion of urban and rural participants beyond the beneficiary sample allowed us to gather data from a more representative Cambodian sample and include a potential “future” vision of how food environment and consumption might change in rural areas with increasing access and availability (as Phnom Penh, the capital, is further along in its nutrition transition).
The study is unable to interpret trends in dietary patterns and nutritional transition, as no baseline or follow-up data are presented, but it does provide a current snapshot of dietary intake and the food environment in Cambodia.
Together, these results show that the food environments in urban and rural Cambodia both include increasingly industrialised (processed) food sources, but to different degrees. This data provides a novel, cross-sectional view of the state of the nutrition transition in Cambodia and provides valuable insights into areas requiring attention from programmes and policies.
For more information, please contact Hillary Fry at hillarylfry95@gmail.com.
References
Bose I, Deptford A, Baldi G et al. (2018) Consumption of empty-calorie snack foods raises cost of nutritious diet. Sight and Life, 32, 2, 29–39.
Consortium for Improving Complementary Foods in Southeast Asia (2023) Cambodia COMMIT Synthesis Report. unicef.org.
Herforth A, Wiesmann D, Martinez-Steele E et al. (2020) Introducing a suite of low-burden diet quality indicators that reflect healthy diet patterns at population level. Current Developments in Nutrition, 4, 12.
Kulikov A, Mehta A, Tarlton D et al. (2019) Prevention and control of noncommunicable diseases in Cambodia: The case for investment. WHO Regional Office for the Western Pacific.
Lipoeto N, Lin K & Angeles-Agdeppa I (2021) Food consumption patterns and nutrition transition in South-East Asia. Public Health Nutrition, 16, 9, 1637–1643.
National Institute of Statistics (2022) Cambodia demographic and health survey 2021-22: Final report. dhsprogram.com.
1 Mobile and street vendors sell fresh produce, sugar-sweetened beverages, and snacks. However, street vendors more commonly have access to refrigeration and may also sell cooked or prepared food.
About This Article
Jump to section
Download & Citation
Reference this page
Hillary Fry and Sanne Sigh (2024) Cambodia: Impacts of the nutrition transition on urban and rural mothers and children. Field Exchange 72. https://doi.org/10.6084/m9.figshare.25460902