
Finding the most vulnerable: Ways to identify malnourished infants
This is a summary of the following paper: Mahmud I, Guesdon B, Kerac M et al (2024) Mortality risk in infants receiving therapeutic care for malnutrition: A secondary analysis. Maternal & Child Nutrition, e13635. https://onlinelibrary.wiley.com/doi/epdf/10.1111/mcn.13635?domain=p2p_domain
This secondary analysis investigated inpatient therapeutic care data for 3,692 infants (aged <6 months) across 34 field sites, between 2002 and 2008, from 12 countries: Afghanistan, Burundi, the Democratic Republic of Congo, Ethiopia, Kenya, Liberia, Myanmar, Niger, Somalia, Sudan, Tajikistan, and Uganda. Admittance criteria was comprised of 1) infant too weak to suckle effectively, 2) not gaining weight at home, 3) weight-for-length z-score <-3, and/or 4) presence of bilateral pitting oedema. Multiple variables were collected at admission and discharge, with death at discharge being the outcome of interest in this analysis. Logistic regression was used to examine the association of various anthropometric deficits and mortality.
In this admitted population, 95.8% were underweight, 82.8% wasted, and 77.8% stunted (figure 1). When applying the Composite Index of Anthropometric Failure (CIAF) – which combines underweight, wasted, and stunted into a single indicator of anthropometric deficits – 96.8% of children fell under this classification. Infants with multiple anthropometric deficits were often more severely wasted, stunted, and underweight than those with a single anthropometric deficit. This underscores the urgent need for targeted interventions to address the specific needs of these vulnerable infants.
Figure 1: Prevalence and overlap of different anthropometric deficits and mortality
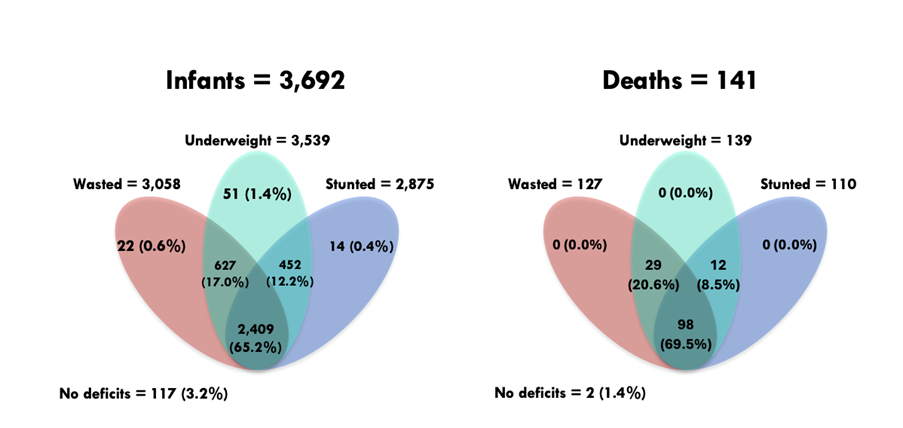
A total of 141 infants died during inpatient therapeutic care, of which 116 were severely wasted and 138 were severely underweight. Severely wasted infants had double the odds of mortality (OR 2.1, 95% CI 1.2-2.7, p=0.009) compared to anthropometrically normal infants. Severely underweight infants had over triple the odds of mortality (OR 3.3, 95% CI 0.8-13.6, p=0.09), although this was not a significant finding due to the broad confidence interval observed. Notably, weight had fewer missing values and flagged data, making this assessment more practical. Sex differences were observed, where boys had greater odds of inpatient mortality than girls (OR 1.40, 95% CI 1.02-1.92, p=0.03). In this analysis, the only infants to die were those with multiple anthropometric deficits, although their odds of mortality were not significant due to the broad confidence intervals observed.
The study excluded participants with missing data and/or outlier data based on predetermined guidelines, which may increase our confidence in the statistical analysis, but may also introduce selection bias into the sample. As this study took place across multiple sites, variation in measurements taken by different staff may have introduced measurement bias. However, the inclusion of multiple sites increases both the sample size and the generalisability of the findings. Seasonality may also affect our interpretation, as measurements were taken at different time points in different locations. This analysis lacked data on participants' co-morbidities, congenital anomalies, prenatal and birth history, or breastfeeding practices. These factors could potentially influence the observed associations between anthropometric deficits and mortality.
These results are not generalisable beyond this inpatient setting – which is a subgroup of already malnourished children – so the findings should be interpreted with caution. This analysis does reinforce existing knowledge that there are sex differences in malnutrition-related mortality and that children with concurrent forms of malnutrition face the greatest mortality risk. Using more comprehensive indicators, such as CIAF, offers a more holistic understanding of undernutrition and risk of infant mortality. Yet, more research is needed to determine the added benefit of CIAF whilst balancing its additional burden/complexity for programme staff. Wasting and underweight appear to correlate more strongly with mortality compared to stunting in this setting.