
Nigeria Governors’ Forum Nutrition Scorecard: routine data for nutrition accountability
This is a summary of a Field Exchange field article that was included in issue 67. The original article was authored by Ahmad Abduwahab, Yashodhara Rana, Oluwagbenga Sadik, Caroline Snead, Grace Agi, Gianni Dongo, Chinekwu Oreh and Rebecca Heidkamp.
Ahmad Abduwahab is the Senior Health Advisor of the Nigeria Governors’ Forum Secretariat.
Yashodhara Rana is an Associate Director at Results for Development.
Oluwagbenga Sadik is a Nutrition Policy Analyst with the Nigeria Governors’ Forum Secretariat.
Caroline Snead is a medical student at the Kaiser Permanente Bernard J. Tyson School of Medicine.
Grace Agi is a nutritionist working with the Nigeria Governors’ Forum Secretariat.
Gianni Dongo is a Public Health Physician and the Nigeria Governors’ Forum Programme Officer for Health.
Chinekwu Oreh is a Health Specialist with the Nigeria Governors’ Forum Secretariat.
Rebecca Heidkamp is a Public Health Nutritionist and Associate Scientist at the Johns Hopkins Bloomberg School of Public Health who leads the DataDENT initiative.
|
Key messages:
|
Background
The Nigeria Governors' Forum1 is a non-partisan platform that uses data to inform decision-making. In 2019, the Forum Secretariat began developing a scorecard tool to track state-specific progress towards the Governors’ commitments to nutrition action. The commitments were to (1) set up or revitalise State Committees on food and nutrition; (2) establish state-specific multi-sector plans for nutrition; (3) increase budgetary spending on nutrition interventions; and (4) promote maternity protection for civil servants.
Between 2019 and 2021, the Nigeria Governors’ Forum Secretariat collaborated with Data for Decisions to Expand Nutrition Transformation (DataDENT2) and other stakeholders including the Federal Ministry of Health to design and implement the nutrition scorecard. The scorecard (Figure 1) was launched in 2021 and is presented semi-annually to the Governors of each state.
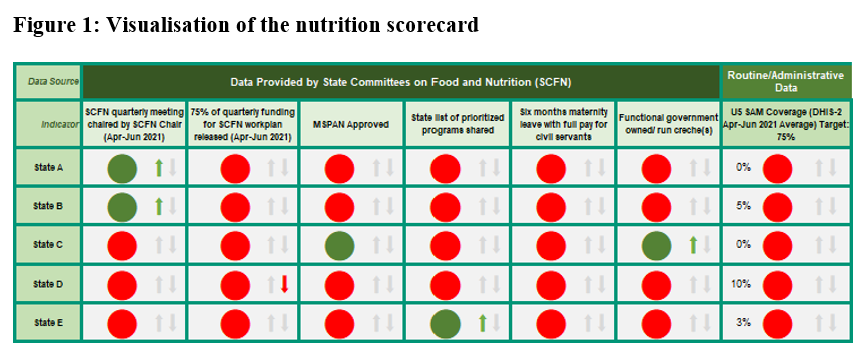
Along with indicators on the four commitments, the scorecard includes a nutrition outcome indicator drawn from the health management information system (HMIS)/district health information software (DHIS2) reports. Using administrative data has several challenges including incomplete and inaccurate reporting, a shortage of data collection instruments and limitations in estimating the target populations for denominators. This article describes how a nutrition outcome indicator was selected for the nutrition scorecard and the challenges faced. It also makes recommendations to improve the usability of HMIS/DHIS2 data.
Process for selecting outcome indicators
The DHIS2 is a web-based software system that facilitates the collection and analysis of health data sourced from the national HMIS. All health facilities in Nigeria complete a monthly summary form using facility-level HMIS registers and the data is shared up administrative levels via the DHIS2 web platform. Reporting rates are generally high, reaching 86.2% in 2019 and 81.9% in 2020.
The selection of DHIS2-derived outcome indicators by the Governors’ Forum and DataDENT teams followed a four-step process:
- The monthly summary form and online DHIS2 dashboard were reviewed to identify available nutrition data elements. The monthly summary format was updated in 2019 but only six states had rolled this out at the time of scorecard design. Thus, only indicators in the previous 2013 version were considered for inclusion.
- Monthly trends were reviewed for all available nutrition indicators from January 2019 to November 2020.
- The list of potential indicators was refined based on (1) the completeness of data; and (2) whether it reflected nutrition outcomes for all children rather than only those seeking care at facilities. Specific attention was given to whether denominators could be constructed to reflect state-level trends.
- The appropriateness of the proposed indicator list was confirmed with nutrition measurement experts and the HMIS/DHIS2 team in Nigeria.
Selected indicators
A number of nutrition indicators were considered during the selection process: severe acute malnutrition (SAM) treatment coverage, vitamin A coverage, exclusive breastfeeding rate, underweight, deworming, SAM recovery and growth monitoring. Based on the review criteria, SAM treatment coverage was selected as the only outcome indicator for the nutrition scorecard. Data was generally complete for this indicator and it was also considered that this indicator could give an indication of the trends for all children. Coverage is calculated quarterly for each state according to the method in Box 1.
Box 1: SAM treatment coverage calculation method
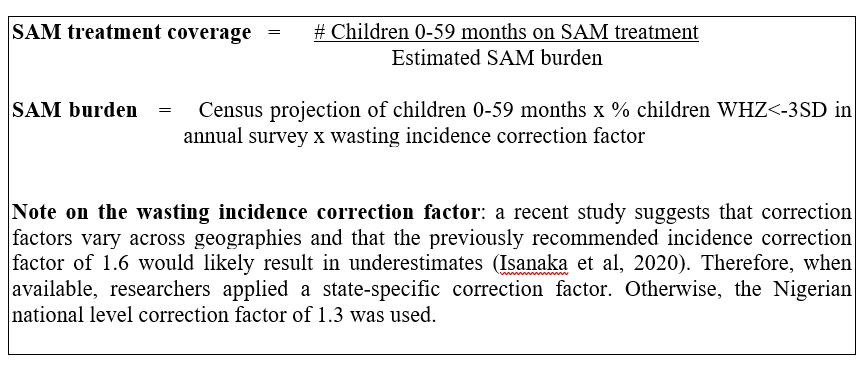
* When available, a state-specific correction factor was used. Otherwise, the Nigerian national level correction factor of 1.3 was used.
Since SAM treatment is almost exclusively delivered through health facilities, the HMIS/DHIS2 system was expected to capture most service delivery to populate the numerator. The denominator, calculated using census population projections and SAM prevalence from annual national surveys, estimates the number of children at risk. Direct estimates of SAM treatment coverage (e.g., Simplified Lot Quality Assurance Sampling Evaluation of Access and Coverage or Simple Spatial Surveying Method) would be more precise but are not feasible at scale. Thus, while estimating the denominator was deemed appropriate, this may have overestimated the burden.
Limitations of using routine data
- Community-level nutrition services may not be adequately captured: Nigeria’s HMIS/DHIS2 system is not designed to capture community-level nutrition services. However, several nutrition interventions such as vitamin A supplementation and deworming are commonly delivered through community-level platforms and events.
- Age-disaggregated data is not always available: The age-disaggregated data needed to estimate the denominators for some coverage indicators (e.g., exclusive breastfeeding rates) is not available in the HMIS/DHIS2 system.
- Data may have quality issues: Some indicators could not be used in the scorecard because too much data was missing or there were anomalous results.
- Delay in the rollout of the 2019 monthly form and facility registers: As previously mentioned, there were delays in rolling out the 2019 monthly form and in updating facility registers. Many potential nutrition indicators were therefore not reported by most states. In addition, there were many months of missing data among states that did use the 2019 form. The Nigeria Governors’ Forum considered using projections to address the data gaps for some indicators in 2020 but this was not viable due to a lack of historical data.
Recommendations to improve the HMIS/DHIS2
- Reflect outreach services in HMIS/DHIS2 reports. This could be achieved by (1) creating outreach event components in HMIS/DHIS2; or (2) aggregating data on the monthly reporting forms of the health facility implementing outreach services.
- Facilitate better estimation of denominators. For example, develop standardised catchment populations for age-specific nutrition services or establish population-informed benchmarks for the absolute number of services delivered per month.
- Include estimates derived from other data sources in the HMIS/DHIS2 system.
- Increase investment in facility-level data quality assessment and assurance activities. These should focus on how to correctly extract and collate data from monthly forms and for entry into the HMIS/DHIS2.
Conclusion
As in many countries, the HMIS/DHIS2 platform is a critical source of routine nutrition data in Nigeria. However, its utility for decision-making depends on overcoming existing shortcomings in data quality and information gaps. The Nigeria Governors’ Forum health team will continue to use HMIS/DHIS2 data for state-level advocacy as well as to engage the Federal Ministry of Health around improving the quality and reliability of the data.
For more information, please contact Ahmad Abduwahab at aabdulwahab@ngf.org.ngf