Scaling up a community-based nutrition package in Afghanistan to improve complementary feeding practices in children 6-23 months of age
 |
Click here to listen to an interview with the author on the ENN podcast channel |
Dr Mohammadullah Noorzad is the Senior Officer for the Community Based Nutrition Programme in the Public Nutrition Directorate, Ministry of Public Health, Afghanistan. He has more than 14 years’ experience in health and nutrition programmes, including operationalising community-based growth monitoring and promotion.
Dr Palwasha Anwari is a Nutrition Programme Officer with UNICEF Afghanistan. She manages infant and young child feeding programmes, including community-based nutrition interventions, and has more than 10 years’ experience in humanitarian and development settings.
Maureen L. Gallagher is Chief of Nutrition for UNICEF Afghanistan. She is a public health specialist with over 15 years’ experience in nutrition programming in Africa and Asia.
Introduction
Infant and child mortality rates in Afghanistan are among the highest in South Asia and poor nutritional status is a significant underlying factor. Nearly two million children under five years old, about four in 10 children, are stunted and an estimated one in 10 are wasted1. Twenty-two percent of children aged 6-23 months receive complementary food with minimum acceptable quality and frequency, which ranges from 5% to 23% in different provinces2.
The Ministry of Public Health (MoPH) has been rebuilding the national health system since 2002, with an emphasis on improving access to essential health and nutrition services. The MoPH developed the Basic Package of Health Services (BPHS) in 2003 and the Essential Package of Hospital Services (EPHS) in 2005 to increase the coverage of health services at both facility and community levels. Since the implementation of BPHS and EPHS, progress in public nutrition has been limited, due to low capacity of BPHS service providers and an absence of specific guidelines.
The Government of the Islamic Republic of Afghanistan and its partners are committed to ending maternal and child malnutrition in the country and recognise the need for a comprehensive, multi-sector response mechanism with technical, financial and political support at all levels, including community level. In this context, the Public Nutrition Directorate (PND) within the MOPH began developing a community-based nutrition package (CBNP) in 2016, with the objective of having one community nutrition package for the whole country. The process started with the review and analysis of existing programmes, materials and methodologies, as partners applied different ones. The review was followed by field visits and a subsequent analysis of lessons learned to inform the harmonisation and standardisation of the CBNP.
This article describes how the PND designed the CBNP to improve the diets and feeding practices of young children and the achievements and challenges experienced in the course of its implementation.
 Community members work together on a village nutriton action plan. © UNICEF/2019/ Rezaee
Community members work together on a village nutriton action plan. © UNICEF/2019/ Rezaee
Community-based healthcare in Afghanistan
A cadre of voluntary community health workers (CHWs) forms the backbone of community-based healthcare in Afghanistan. The CHWs deliver basic health and nutrition services from their homes, which are recognised as health posts. These services include maternal and newborn health; child health and immunisation and public nutrition services, such as support for exclusive breastfeeding; community food demonstrations; and community-based management of acute malnutrition. Each health post is operated by a male and female pairing3 to respect culture and community norms and to assist mobility of female CHWs in their communities. There are more than 28,000 CHWs, each responsible for a cluster of 100-150 families, covering 60-70% of communities in the country. The CHWs are mentored and supervised by community health supervisors, who are based at the nearest health facility. A health shura (committee) supports activities in the community and selects, supports and monitors CHW activities. Family health action group members serve as a support group for female CHWs and promote utilisation of health and nutrition services4. There are more than 4,000 family health action groups and around 1,300 community health supervisors nationwide.
The CBNP approach
The CBNP was designed and introduced in 2018 to improve access to essential nutrition services and to improve child feeding practices and diets. It builds on existing community-based healthcare platforms in Afghanistan to deliver nutrition services at community level, as an adjunct to health facility services. The approach has a particular focus on children under two years old, their mothers and fathers, and other male community members who are the main decision-makers at household level.
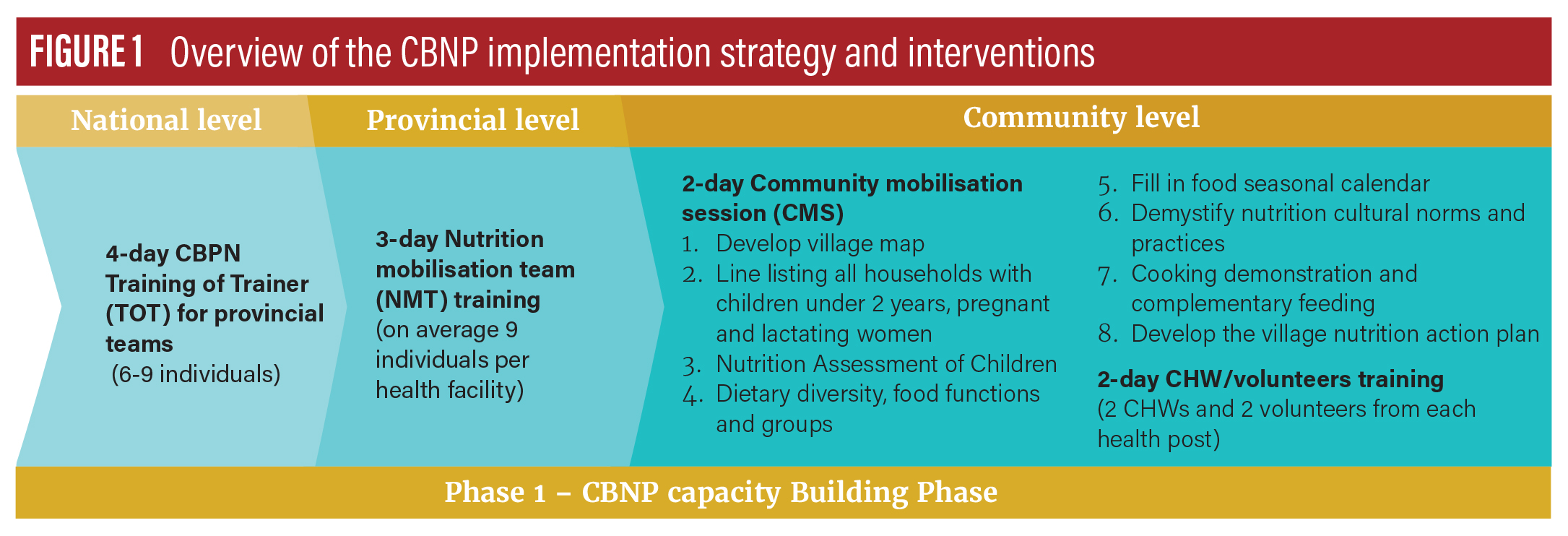
The design of the CBNP is based on a combination of the positive deviance/hearth model and other approaches being implemented in Afghanistan. The programme is initiated in a community through a two-day community mobilisation session, during which community members map their communities, listing all children under two years of age, complete seasonal food calendars and develop a village nutrition action plan (see Figure 1 – Community level). These sessions are led by nutrition mobilisation teams, usually drawn from existing community-based platforms from other sectors, recognising the importance of a multi-sector, systems-based approach for improving infant and young child feeding (IYCF) at community level5.
The first step in community mobilisation under the CBNP is to develop a village map to identify all households with children under two years of age and make a nutrition assessment of those children. Parents of children whose mid-upper arm circumference (MUAC) is in the ‘green zone’ are identified as role models. These parents are requested to engage with the community and share their positive child-feeding practices with other parents and demonstrate the adoption of similar practices. In terms of home visits and food-demonstration sessions, CHWs give priority to households with children in the ‘yellow’ or ‘red’ MUAC zones and facilitate learning from other mothers. As per standard protocol, children with red MUAC (below 11.5 cm) are referred to health facilities for treatment of severe acute malnutrition.
Participatory tools to improve young children’s diets
The CBNP delivers a number of focused interventions for improving young children’s diets and feeding practices. Several participatory methodologies and tools (developed during the community mobilisation sessions) are used to support delivery of these interventions, including:
- Seasonal food calendar tool is used to explore and map the available foods during different seasons of the year. It is used to encourage consumption of these locally available foods based on availability across the seasons.
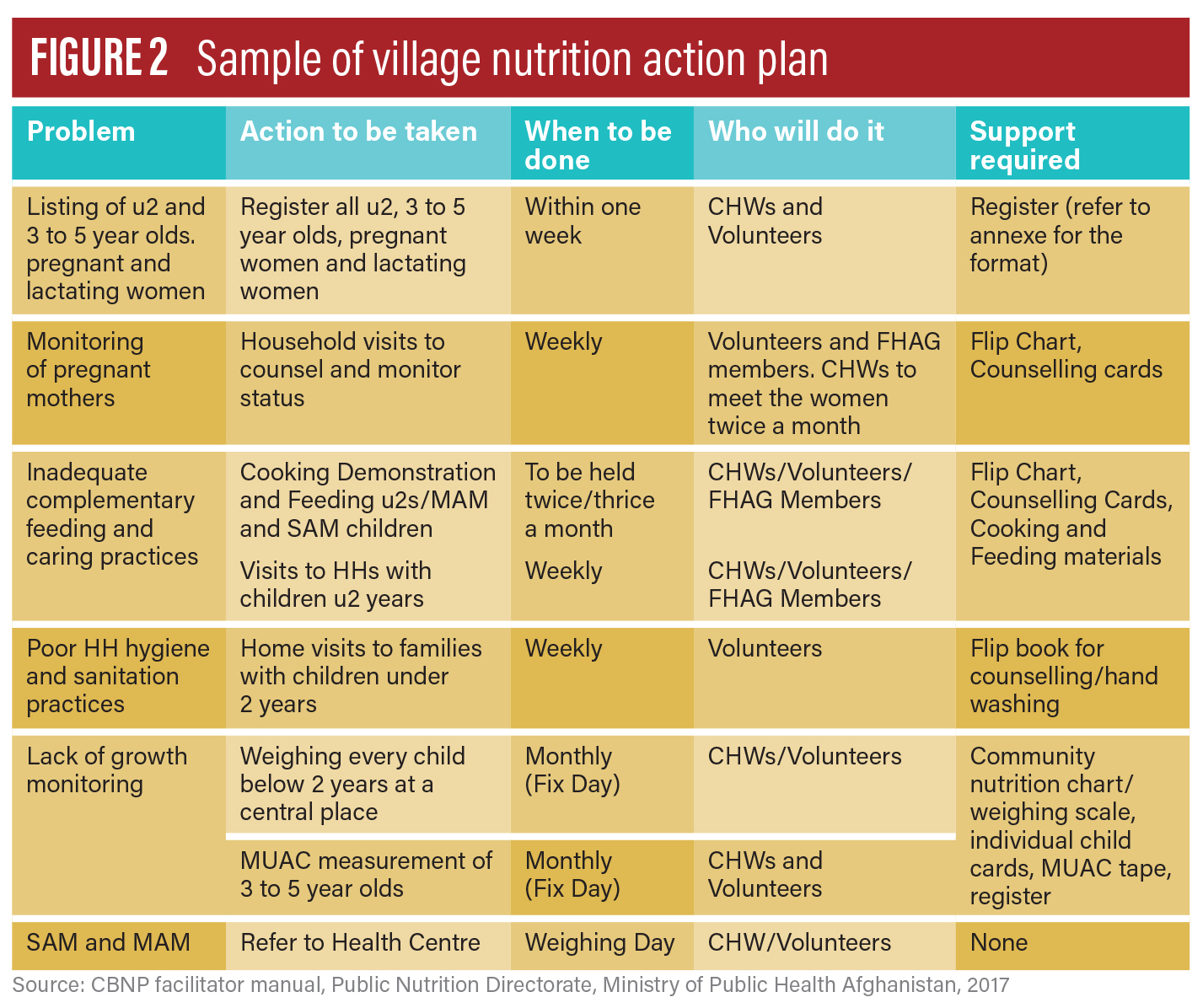
- Village nutrition action plans (see Figure 2) focus on improving the nutrition status of families; particularly those with children under two years of age (described below). The plan is developed by community members based on the discussion and assessment of their children’s nutrition status. They are asked to identify a few critical actions to tackle and prevent malnutrition in their communities. Members of the health shura, community health supervisors and CHWs are responsible for tracking implementation of the action plan.
- Food demonstration sessions teach families with children under two years old about the preparation of complementary foods by using different available food groups.
Towards the end of the two days, the communities identify two additional volunteers (a male and a female for gender balance and as key influencers for both sexes) to support CHWs in the implementation of the CBNP.
Capacity-building and implementation phases
The CBNP rollout at provincial level has two distinct phases: Phase One for capacity-building and Phase Two for implementation. Phase One comprises a series of cascading training activities, beginning with the training of provincial master trainers at the national level down to selection of a number of community volunteers to serve in nutrition mobilisation teams (see Figure 1).
Phase Two focuses on a participatory process for the development of detailed guidelines for implementing the activities identified by communities under the village nutrition action plan, recognising the key role of CHWs in the implementation of the plan and activities.
From design to implementation: Building programme success
The initial focus has been on implementation of CBNP capacity-building in 2019 in four provinces with the worst child nutrition indicators. The initiative had reached about 2,000 health posts, around 8,000 CHWs and community volunteers, and more than 84,000 community members, both male and female, by the end of 2019. Data from the four provinces where the capacity-building phase is complete demonstrates potential effective community engagement and increased awareness of IYCF, although it is too early to measure the impact of the CBNP in improving young children’s diets and feeding practices. However, an analysis of routine health data shows that the coverage of home visits by CHWs has increased by 5-10 percentage points, while the number of growth-monitoring promotion (GMP) sessions has increased considerably (for example, by up to 90% in Takhar province), indicating increased programme reach (REF). Both home visits and GMP sessions offer crucial opportunities for contact with caregivers and for increasing the coverage of counselling support in improving diets and feeding practices. These results indicate that the CBNP has provided participatory tools for CHWs to increase interactions with target families to deliver nutrition education, and cooking demonstrations, counselling and screening to facilitate prioritisation of actions.
BOX 1: Comments from a CHW
“CBNP is a successful approach as it is based on community needs. All programme materials are pictorial [which enables] me to easily understand, with limited literacy. Besides that, there are practical food demonstration sessions for mothers on feeding young children – complementary feeding. I noticed how much mothers of children under two years old happily have participated and contributed in food demonstration sessions. I learned how to assess malnourished children by weighing scales and MUAC. I encourage mothers on timely introduction of diverse diets to children over six months old. I conduct weekly follow-up of children with yellow MUACs and observe their feedings at their homes. I observed positive changes in my village. Here, there was a common practice of not giving eggs to young children, thinking that was not good for them. Now, I see that mothers give a well-cooked egg to their young children, beside breastmilk.” Ms. Benazir, female CHW (since 2005) from Pul-e-Khumri District, Baghlan Province
Scaling up CBNP
CBNP has scaled up rapidly to 19 out of 34 provinces within two years by utilising the existing community-based healthcare platforms. For Phase One (capacity-building), an off-budget annual cost of about USD 700 to USD 900 per health post is estimated. In Phase Two (implementation), minimal financial outlay is required, with costs to be covered by service providers who have contracts with the government, if CBNP is integrated into the community package. PND and its technical partners, including the United Nations Children’s Fund (UNICEF), continue efforts to mobilise resources to scale up CBNP in all remaining provinces and advocate for its integration into the health package.
Addressing challenges
A number of delivery constraints have been noted. Findings from the process evaluation and CBNP annual programme reviews indicate that some critical community mobilisation activities using participatory tools, such as seasonal food calendars, food demonstration sessions and village nutrition action plans, were not implemented as per the guidelines. The CBNP was viewed as an approach focused mostly on supporting early case detection of SAM children for treatment and care, rather than promoting preventive measures to improve diets and feeding practices. This could be attributed to the rapid scale-up of implementation, which did not enable strong community and household engagement. Also, household-level factors such as food availability and accessibility could have posed constraints on the ability of households to put into practice required behavioural changes and feeding practices, thus negatively impacting engagement with the CBNP. The package and approach are being revised to integrate recommendations for better uptake of preventive measures.
The CBNP is also facing several coverage challenges, particularly accessibility to remote areas due to harsh terrain and climate, and ongoing insecurity. In addition, the workload of CHWs is a concern, particularly as they are volunteers and have responsibilities for delivering a broad range of health and nutrition services, such as family planning, treatment of child illnesses, tuberculosis, GMP, and others.
UNICEF supports PND in advocating with the MoPH leadership and health donor agencies, such the World Bank, the European Commission, USAID and Canada, for incentivising CHW performance. In Afghanistan, the MoPH has contracted out health service provision to non-governmental organisations (NGOs), who are the service providers. Payment of NGOs uses a payment-for-performance (P4P) financing model, based on achievement of targets for certain identified indicators. While community nutrition activities are part of BPHS services, there are no community nutrition indicators in the P4P results-monitoring framework. This contributes to weak accountabilities; as a result, BPHS service providers do not give enough attention to implementing community nutrition services. PND and its technical partners are advocating to include at least one community nutrition indicator in the set of P4P indicators. This could help build greater accountability of delivery of community nutrition services and ensure the sustainability of the CBNP initiative.
Conclusion and next steps
The CBNP approach went to significant scale in a short period of time. Lessons learned from rolling out CBNP in more than half of Afghanistan’s provinces over the last two years and findings from the process evaluation (concluded in mid-2020) will be used to support a review of implementation strategies and approaches and inform the design of the next phase of the rollout. An endline study in 2022 will provide evidence on the impact of the CBNP on complementary feeding practices. The platform created by CBNP has much potential to improve the diets of young children, especially as the approach is evaluated and refined.
Footnotes
2National Nutrition Survey (2013) Ministry of Public Health, Afghanistan.
3This could be a husband and wife, as well as a mother and son or brother and sister.
4Community-based Healthcare Strategy (2015-2020), Ministry of Public Health, Afghanistan.
5Nutrition mobilisation teams may be drawn from community-led total sanitation (CLTS) members from the water, sanitation and hygiene (WASH) sector, agricultural extension officers from agriculture/food systems, selected shura members, and resources personnel from the health system.